서 론
위는 위 내 산성 환경, 풍부한 혈류와 위배출, 항균성 단백질 등의 방어기전으로 인해 병태생리적으로 세균 감염이 일어나기 어려운 장기이다[1,2]. 헬리코박터 파일로리(Helicobacter pylori , H. pylori)는 요소분해효소를 분비하여 위산으로부터 자신을 보호해 위 내 방어기전을 회피할 수 있어 세균성 위 감염의 주요 원인으로 잘 알려져 있다[3]. 위산으로부터 방어기전을 갖추지 않은 H. pylori 이외 대부분의 세균에 의한 위 감염은 매우 드물고, 내시경 소견도 특이적이지 않아 진단이 쉽지 않다[3,4]. 결과적으로 치료가 지연되거나 다른 악성질환과 감별을 위해 수술을 진행하는 경우도 있다[5]. 본 글에서는 H. pylori 이외 드물지만 국내에서 발생할 수 있는 4가지 세균성 위감염 질환인 급성 봉소염성 위염, 위매독, 위결핵, 위 방선균증의 내시경 소견 및 진단과 치료에 대해 기술하고자 한다.
본 론
급성 봉소염성 위염(acute phlegmonous gastritis)
급성 봉소염성 위염은 위 점막하층의 세균성 감염을 시작으로 위전층(transmural)에 위부종이나 괴사가 발생할 수 있는 드물지만 치명적인 질환이다[6,7]. 급성 봉소염성 위염은 1820년에 Cruveilhier 등에 의해 최초로 기술되었으며, 전 세계적으로는 500건 이상이 보고 되었다[8,9]. 급성 봉소염성 위염은 1919년 항생제가 발견되기 전에 보고된 시기에는 사망률이 약 92%에 달했으며, 항생제가 발견된 이후인 1973-2003년까지의 보고에서는 이전에 비해 많이 나아졌다고는 하지만 여전히 42%로 높은 사망률을 보인다[8]. 만성적인 음주력, 만성신부전, 조절 불량 상태의 당뇨, 면역저하 등의 위험 요인을 가진 환자에서 점막 손상 부위를 통한 세균 감염이 병의 기전으로 제시되고 있다[6-8,10,11]. 최근에 증가하고 있는 내시경 절제술로 인한 점막 결손뿐만 아니라 조직검사 또는 내시경 초음파(endoscopic ultrasonography)를 통한 미세침흡인검사(fine needle aspiration)와 같은 미세한 점막 손상 이후에도 급성 봉소염성 위염이 발생한 증례들이 보고된 바 있다[11-16]. 급성 봉소염성 위염의 주요 원인균으로는 Streptococci가 있으며, 전체 감염 중 약 70%-75%를 차지한다. 또한, Staphylococci , Escherichia coli , Haemophilus influenza , Proteus, Clostridia와 같은 균들도 위 생검 조직이나 위액 배양에서 확인될 수 있다[7,8,17]. 가스를 형성하는 균에 의한 감염의 경우 위벽에 공기가 형성되는 기종성 위염(emphysematous gastritis) 으로 나타날 수 있다[8]. 또한, 괴사성 위염(necrotizing gastritis)은 급성 봉소염성 위염의 가장 치명적인 형태로, 점막하 혈관에 광범위하게 형성되는 혈전이 특징이다[8]. 괴사성 위염은 위벽이 괴사되면서 복막염으로 빠르게 진행할 수 있어서, 진단이 지연되거나 간과될 경우 사망률이 높다[15,18].
내시경 소견
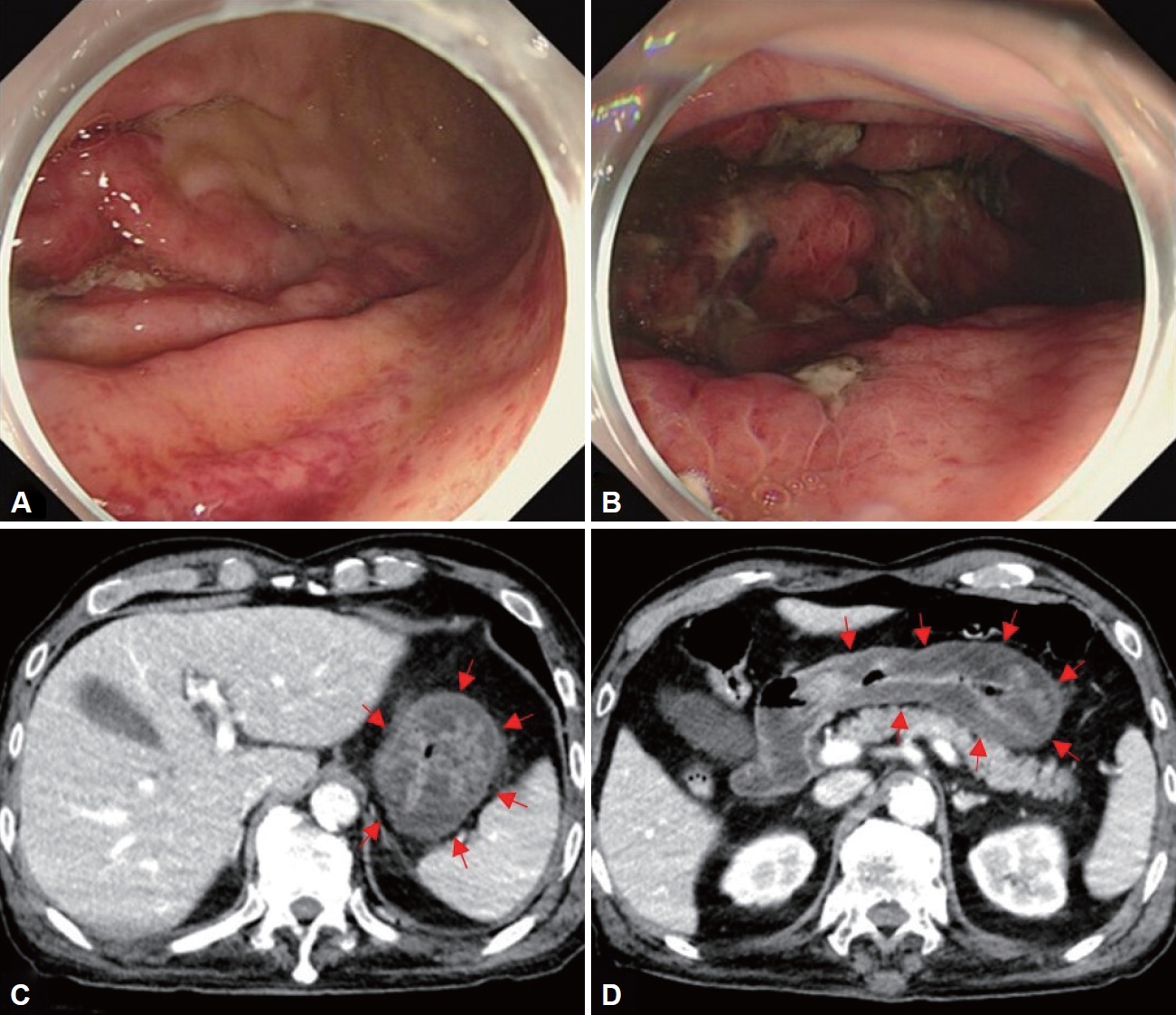
급성 봉소염성 위염은 침범 범위에 따라 국소형과 미만형으로 나눌 수 있는데, 국내 보고에서는 미만형이 더 흔하게 관찰되었다. 내시경 소견으로 점막 발적, 부종, 화농성 삼출물이 동반된 궤양이나 농양 등이 관찰될 수 있다(Fig. 1A and B). 위 전벽의 기능 저하로 위마비가 생기면 충분한 금식 기간에도 불구하고 저류된 음식물이 관찰될 수 있다[6].
영상 소견
복부 전산화 단층촬영(computed tomography)을 통하여 두껍고, 저음영의 위벽을 관찰할 수 있으며(Fig. 1C and D), 위벽 내 농양이 보이는 경우도 있다[6]. 초음파 내시경은 복부 전산화 단층촬영에 비해 위벽의 두께 및 염증파급정도를 평가하는데 유리하다[20]. 초음파 내시경에서 위벽이 미만성(diffuse) 으로 두꺼워져 있고, 저음영의 점막하층이 관찰될 수 있는데 이는 말트림프종(mucosa-assisted lymphoid tissue lymphoma) 초음파 내시경 소견과 비슷해 보일 수 있지만, 임상양상과 내시경 소견으로 감별이 가능하다[8].
진 단
복통 및 감염의 징후를 보이는 환자에서 내시경 소견 및 복부 전산화 단층촬영을 통해 의심해 볼 수 있고, 점막 및 점막하 생검 조직에 대해 그람 염색(gram stain) 및 세균 배양이 감염의 확진 및 원인균 동정에 도움이 된다[6,7,21]. 검사 시 주의사항으로 위점막 방어벽이 회복되지 않은 상태에서 내시경 검사를 하는 동안 주입된 공기로 인해 증가한 위내 압력이 혈관을 통한 세균의 역류를 유발해 패혈증(sepsis)을 일으킬 수 있다는 증례 보고가 있다. 따라서 급성 봉소염성 위염 환자에서 내시경을 시행할 때는 최소한의 공기 주입만 하고 검사 시간을 줄이려는 노력이 필요하다[14].
치료 및 예후
급성 봉소염성 위염은 1/3에서 복합균 감염이 발생하므로 초기 치료에는 3세대 세팔로스포린과 메트로니다졸 또는 피페라실린-타조박탐 또는 카바페넴 등의 광범위 항생제의 경험적 투여가 필요하다[8,17]. 중증의 환자가 아닌 경우 내과적 치료만으로 완치된 사례가 보고되었으며, 항생제 투여와 함께 내시경적 미세침흡인술을 통해 위벽 내 농양을 배농하여 수술 없이 완치된 사례도 있다[22]. 하지만 37명을 대상으로 한 보고에 따르면 질병이 미만성으로 파급된 환자 중에서 보존적인 치료를 받은 경우의 사망률은 60%였고, 오히려 수술적 치료를 받은 경우의 사망률은 33%였다[8]. 따라서 항생제 치료를 지속하는 중에 환자의 상태가 악화된다면 적극적인 수술적 치료를 고려하는 것이 필요하다[8].
위매독(gastric syphilis)
매독은 성매개감염으로 spirochete class에 속하는 Treponema pallidum에 의해 발생한다[23]. 국내에서는 2019년 매독 전수감시에서 1753명의 환자 발생이 보고되었으며, 이 중 남성은 1276명(72.9%), 여성은 474명(27.1%)이었다. 연령별로 20-40대가 1281명(73.2%)으로 많았으며, 60세 이상은 192명(11.0%)이었다. 병기별로 1기 매독은 1176명, 2기 매독은 554명, 선천성 매독은 23명 보고되었다[24]. 위매독은 보통 2기 매독에서 발생하며, 전체 매독 환자의 1% 미만에서 발생한다[25,26]. 52명의 위매독 환자를 분석한 보고에 따르면 남자가 많았으며(63%), 평균연령은 39세였고, 과거에 매독을 진단 받았던 경우는 13%에 불과했다[26]. 위매독은 매독 병력에 대한 문진만으로 배제할 수 없고, 임상 소견이 비특이적이어서 의심하지 않으면 진단하기 어렵다. 특히 내시경소견, 병리소견도 위암이나 림프종과 비슷한 양상으로 나타날 수 있어서 진단에 어려움이 있다[26-28].
임상 소견
위매독은 철저한 병력 청취를 통해 매독 병력, 성매개감염(sexually transmitted infection) 위험요인 등의 확인이 필요하다. 위매독의 증상 중에서는 상복부 통증이 가장 흔하며, 그 다음으로 오심과 구토 증상이 빈번하게 나타난다. 토혈, 흑색변, 빈혈과 같은 상부 위장관 출혈소견이나 조기 포만감, 체중감소가 나타나는 사례도 있었다[26,29]. 신체 검진에서는 33%의 환자에서만 매독 징후가 관찰되었으며, 발진(65%), 림프절 병증(53%), 성기 궤양(35%) 순으로 빈도가 높았다[26]. 일부 환자에서만 매독 징후를 발견할 수 있기 때문에 정상적인 신체진찰만으로 위매독을 배제할 수 없다[5,30].
내시경 소견
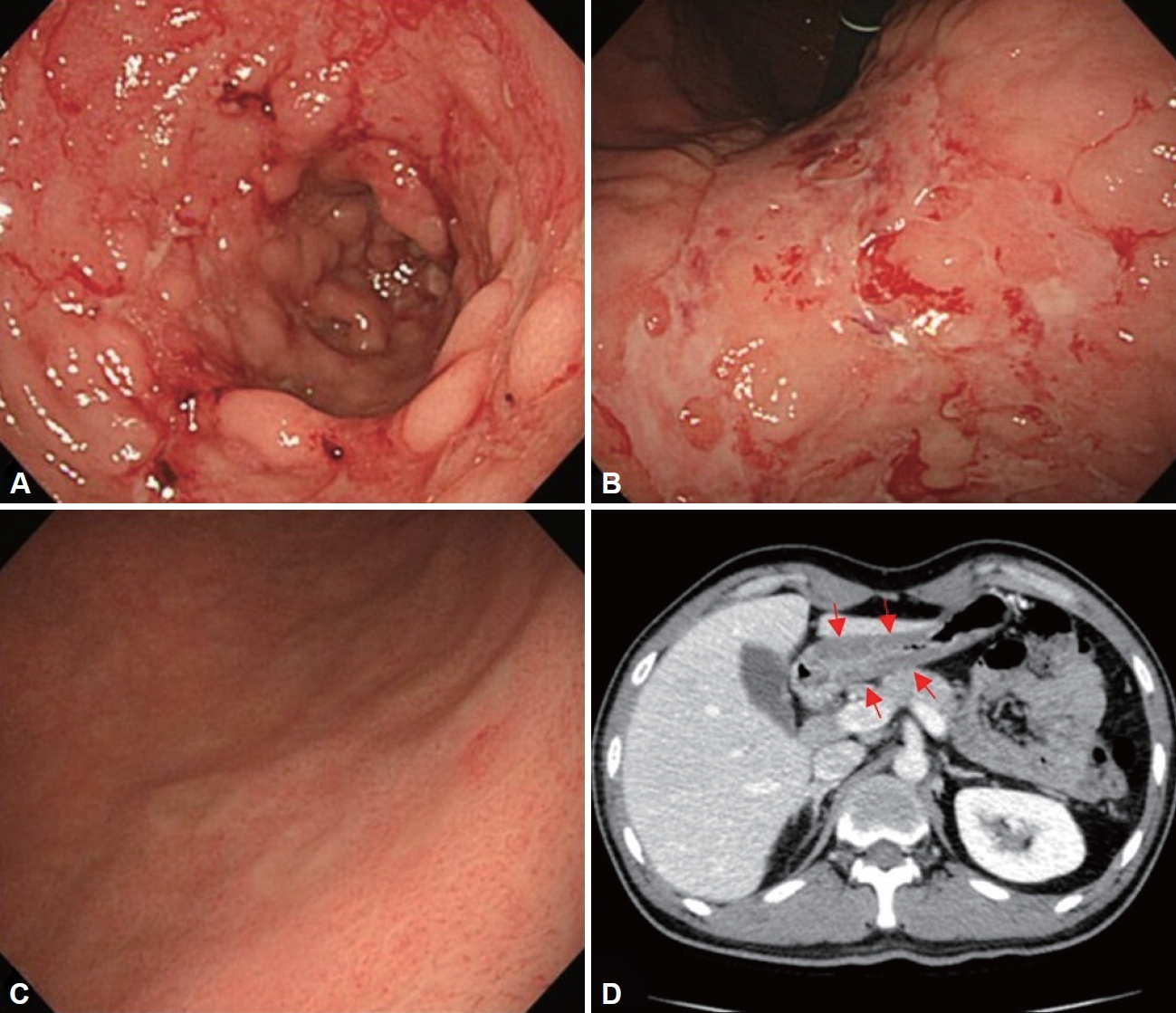
위매독의 주된 호발 부위는 전정부와 위각부, 원위부 체부이며, 상대적으로 위 기저부나 십이지장은 잘 침범하지 않는다[26,31]. 내시경 소견으로는 다발성 궤양, 거대 궤양, 미란, 두꺼워진 점막 주름, 결절성(nodular) 점막, 종괴(mass), 협착(stenosis)의 형태를 보일 수 있으며, 여러 형태의 병변이 혼재되어 있는 경우가 많다(Fig. 2A and B) [5]. 동전 모양의 구진(papule) 이 나타나면 위매독을 가장 우선적으로 고려해 볼 수 있다(Fig. 2C). 내시경적으로 결핵, 크론병(crohn’s disease), 사르코이드증(sarcoidosis), 보만 4형 위암(borrmann type 4), 림프종, 호산구성 위염(eosinophilic gastritis) 등과 비슷한 형태를 보일 수 있다[26,29,32,33]. 제산제 치료에도 치유되지 않는 궤양(refractory ulcer)이나 비전형적인 점막 변형을 가진 병변에서 진단이 안될 때 위매독을 의심을 해볼 수 있다[5].
진 단
매독의 혈청학적 검사로는 두 종류, 비트레포네마 검사(non-treponemal test)와 트레포네마 검사(treponemal test) 가 있다. 한 가지 종류의 검사만 시행한다면 위양성(falsepositive) 결과를 포함하여 최근 감염과 오래된 감염을 구별할 수 없기 때문에 두 가지 종류의 검사를 모두 시행한다. 선별검사로 주로 사용되는 비트레포네마 혈청학적 검사에는 rapid plasma regain test, venereal disease research laboratory 검사가 있고 지질 항원에 대한 항체를 측정하는 방법이다. 양성 검사 결과는 정량적 역가로 보고되며, 이는 질병의 활성도와 관련이 있다. 트레포네마 혈청학적 검사에는 fluorescent treponemal antibody absorption, T. pallidium latex agglutination, enzyme immunoassay 검사법 등이 있다. IgM은 후기 매독이나 치료받은 매독에서는 주로 음성이며, IgG는 치료받은 매독에서도 평생 양성이다. 매독에 대한 트레포네마와 비트레포네마 검사 모두에서 위양성 반응이 나타날 수도 있다. 위양성 결과의 가장 일반적인 원인은 고령, 자가면역질환, 심혈관계 질환, 임신, 말라리아, 다른 spirochete 감염 및 최근의 예방접종이 있다. 확진을 위해서는 위병변의 삼출물 또는 조직검사에서 트레포네마균을 검출하는 것이 필요한데, 은염색을 통해 spirochete를 확인할 수 있다[34]. 직접 형광항체검사(direct immunofluorescence staining)를 통해 검체에서 트레포네마 항원을 검출할 수 있는 방법은 민감도, 특이도가 높고 비교적 값이 싸면서 결과가 48시간 내에 나오는 장점이 있다[5]. 진단적 민감도를 향상시킬 목적으로 실시간 중합효소연쇄반응검사(real-time polymerase chain reaction) 를 사용할 수 있지만, 20% 정도의 위양성률이 함께 보고되고 있어 해석에 주의가 필요하다. 위매독 병변 조직의 haematoxylin-eosin (H&E) 염색 시 대부분 플라즈마 세포나(plasma cell), 림프구의 침윤으로 인한 미만성 위염이 관찰되며 궤양이 동반될 수 있다. 혈관염은 매독 침범의 특징적인 소견이지만, 혈관이 위치하는 점막하층 검체가 필요하다. 이를 위해 내시경적 점막 절제술(endoscopic mucosal resection) 이나 탐색적 개복술(explorative laparotomy)을 통해 위 매독을 진단한 사례 보고도 있다[5]. 조직검체에서 림프상피병변(lymphoepithelial lesion)과 상피세포 핵의 비전형(nuclear atypia)을 보이는 경우에는 위암이나 위림프종으로 오인할 수 있다[28]. 조직검사에서도 확진이 어려운 경우 혈청학적 검사 소견을 확인하고 경험적으로 항생제를 투여한 후, 단기 추적 관찰하면서 증상 호전 및 내시경적 병변 소실 여부를 종합해서 진단할 수 있다[4].
위결핵(gastric tuberculosis)
폐결핵 환자 0.5% 미만에서 속발성으로 위결핵이 발생할 수 있으며, 결핵균의 섭취로 인하여 직접적인 점막의 감염이 일어나거나, 혈행성 확산(hematogenous spread), 복강 내 임파절을 포함한 주변 장기로부터 전파로 인해 발생한다. 폐 또는 다른 위장관 침범 없이 위에서만 발생한 사례도 있으나 매우 드물다[35,36].
우리나라와 같이 결핵 유병률이 아직 높은 지역에서는 면역억제자가 아니라 하더라도 내시경 소견상 미만성의 침윤성(infiltrative) 병변이나 불응성 궤양, 위출구 협착, 폐쇄 등이 관찰되면 위결핵을 고려해야 한다[37].
내시경 소견
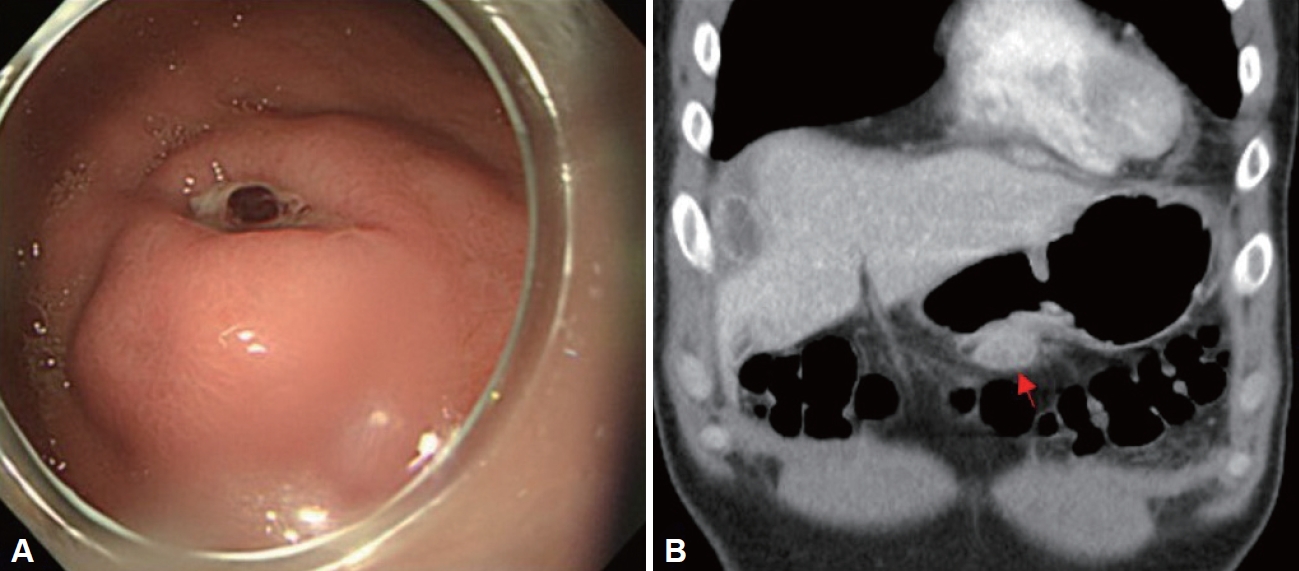
위결핵의 내시경 소견은 비특이적이며 점막의 비후나 발적, 불규칙적인 미란, 궤양 등으로 관찰될 수 있다. 따라서 이러한 형태의 병변을 보일 수 있는 소화성 궤양, 크론병, 매독, 림프종, 사르코이드증 등과 감별이 필요하다. 또한 위점막하 종양(submucosal tumor)과 유사한 형태로 나타날 경우 위점막하 유사 위암이나 위간질성종양(gastrointestinal stromal tumor)과 감별이 필요하다(Fig. 3A) [41]. 위 전층으로 염증이 심해지면 담관 또는 다른 위장관으로 누공(fistula)이 생기기도 한다[42].
진 단
조직 검체의 Ziehl-Neelsen 염색에서 막대 모양의 항산균(acid-fast bacilli)이 염색되거나 건락화된 육아종(caseating granuloma) 소견 또는 랑게르한스 거대세포(Langerhans giant cell)가 확인되면 위결핵으로 진단할 수 있다. 하지만 전형적인 결핵 소견이 나타나지 않는 경우가 많으며, 특히 병변이 점막하층에 깊게 위치하는 경우 육아종 확인 및 항산균 발견이 어려운 경우가 있다. 따라서 충분한 조직검사와 함께 조직을 통한 균 배양과 결핵 중합효소연쇄반응검사를 함께 진행하는 것이 추천된다[43].
위 방선균증(gastric actinomycosis)
위 방선균증은 구강, 위장관, 비뇨생식기관에 상재하는 그람양성이며, 혐기성 균인 Actinomyces israelii에 의해 발생하는 만성 화농성, 육아종성 질환이다[47]. Actinomyces israelii는 손상된 점막에 침투하여 화농성 염증 반응을 유발하며, 결과적으로 농양 및 농루를 형성한다. 위는 위산으로 인해 방선균의 침입과 성장을 막기 때문에 원발적인 위 방선균증은 매우 드물고 수술 후 혹은 고령의 장기간 제산제 복용자, 면역억제자 등에서 발생한다[48,49].
결 론
H. pylori 이외 위의 세균성 감염은 드물고, 비특이적인 임상소견을 보이기 때문에 의심하지 않으면 진단하기 어렵다. 따라서 비특이적이더라도 강도가 심한 위장관 증상을 호소하는 환자는 상부 내시경 검사 전 면역 상태에 영향을 줄 수 있는 환자의 임상 정보 등을 적극적으로 파악하고 검사를 시행해야 한다. 또한 진단을 내리기 어려운 비전형적인 내시경 및 임상양상을 가진 경우에는 다시 충분한 병력 청취와 신체 진찰을 해야 한다. 그리고 내시경 및 영상소견, 혈청학적 검사, 병리검사에 대해서 다시 검토하고 마지막으로 치료에 대한 반응을 종합해 최종적으로 진단해야겠다. 본고에서 서술한 H. pylori 이외 세균성 위감염의 임상적 특징을 표로 비교해보면 다음과 같다(Table 1). 진단 지연은 환자의 삶의 질 저하, 사회비용적인 부담을 높일 뿐 아니라 때로는 치명적인 결과를 낳을 수 있기 때문에 본고에서 언급한 질병들에 대해서 숙지해야겠다.