ņä£ ļĪĀ
ļ╣äņĀĢļ¦źļźś ņāüļČĆņ£äņןĻ┤Ć ņČ£Ēśł(non-variceal upper gastrointestinal bleeding, NVUGIB)ņØĆ ņØ╝ļ░śņĀüņ£╝ļĪ£ ņ×ģņøÉ ļ░Å ņØæĻĖē ļé┤ņŗ£Ļ▓ĮņØä ĒĢäņÜöļĪ£ ĒĢśļ®░, ļåÆņØĆ ņØ┤ĒÖśņ£©Ļ│╝ ņé¼ļ¦ØļźĀņØä ļ│┤ņØĖļŗż[1]. NVUGIBņØś ņŻ╝ļÉ£ ņøÉņØĖņØĆ ņåīĒÖöņä▒ ĻČżņ¢æņØ┤ļ®░, ņØ┤ļŖö ņĀäņ▓┤ ņé¼ļĪĆņØś 50%-60%ļź╝ ņ░©ņ¦ĆĒĢśĻ│Ā, ņØ┤ņÖĖņŚÉļÅä Dieulafoy ļ│æļ│Ć, ĒśłĻ┤ĆņØ┤ĒśĢņä▒ņ”Ø, ņóģņ¢æ ļō▒ļÅä ņøÉņØĖņØ┤ ļÉĀ ņłś ņ׳ļŗż[2,3]. ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ņĀ£ĻĘĀņ╣śļŻīĻ░Ć ļ│┤ĒÄĖĒÖöļÉśļ®┤ņä£ ņ£Āļ│æļźĀņØ┤ Ļ░ÉņåīĒĢśļŖö ņČöņäĖļź╝ ļ│┤ņØ┤Ļ│Ā ņ׳ņ£╝ļ®░, ņ¢æņä▒ņ×É ĒÄīĒöäņ¢ĄņĀ£ņĀ£(proton pump inhibitor, PPI)Ļ░Ć ļäÉļ”¼ ņé¼ņÜ®ļÉ©ņŚÉ ļö░ļØ╝ ņåīĒÖöņä▒ ĻČżņ¢æņ£╝ļĪ£ ņØĖĒĢ£ ņČ£ĒśłļźĀļÅä ņżäņ¢┤ļōż Ļ▓āņ£╝ļĪ£ ņśłņāüļÉ£ļŗż[4]. ņŗżņĀ£ļĪ£ ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ 2006ļģäļČĆĒä░ 2015ļģä ņé¼ņØ┤ ņŚ¼ņä▒ņŚÉņä£ļŖö ļ│ĆĒÖöĻ░Ć ņŚåņŚłņ£╝ļéś ļé©ņä▒ņŚÉņä£ ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£ĒśłņØś ņ£Āļ│æļźĀņØĆ Ļ░ÉņåīĒĢ£ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[5]. ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ ņĄ£ĻĘ╝ 10ļģäĻ░ä ļģĖņØĖņĖĄņŚÉņä£ ņåīĒÖöņä▒ ĻČżņ¢æ ņ¦łĒÖś(peptic ulcer disease, PUD)ņØś ņ”ØĻ░Ć ņČöņäĖĻ░Ć Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░, ĒŚ¼ļ”¼ņĮöļ░ĢĒä░ ĒīīņØ╝ļĪ£ļ”¼ Ļ┤ĆļĀ© ĻČżņ¢æņØĆ Ļ░ÉņåīĒĢ£ ļ░śļ®┤, ņĢĮļ¼╝ Ļ┤ĆļĀ© ļ░Å ĒŖ╣ļ░£ņä▒ PUDļŖö ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ļŗż[6]. ņØ┤ņÖĖņØś ĒŖ╣ņ¦Ģņ£╝ļĪ£ ĻĄŁļé┤ņŚÉņä£ ņåīĒÖöņä▒ ĻČżņ¢æ ļ░Å ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£ĒśłņØĆ Ļ│äņĀłņĀüņ£╝ļĪ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļ®░ Ļ▓©ņÜĖĻ│╝ ļ┤äņŚÉ Ļ░Ćņן ĒØöĒĢśļ®░ Ļ░ĆņØäĻ│╝ ņŚ¼ļ”äņŚÉļŖö ļ╣äĻĄÉņĀü ļō£ļ¼Ė Ļ▓āņ£╝ļĪ£ ņĢīļĀżņ¦äļŗż[7].
ņĄ£ĻĘ╝ ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, NVUGIBļĪ£ ņØĖĒĢ£ ņ×ģņøÉ ĒÖśņ×ÉņØś ņĢĮ 30%ņŚÉņä£ ņ×¼ņČ£ĒśłņØ┤ ļ░£ņāØĒ¢łņ£╝ļ®░, ņØ┤ļ¤¼ĒĢ£ ņ×¼ ņČ£Ēśł ĒÖśņ×Éļōż ņżæ 37.5%Ļ░Ć ņé¼ļ¦ØĒĢ£ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[8]. ņØ┤ļŖö ņØĖĻĄ¼ņØś Ļ│ĀļĀ╣ĒÖöņÖĆ ņŗ¼ļćīĒśłĻ┤Ć ņ¦łĒÖśņØś ņ”ØĻ░ĆņŚÉ ļö░ļźĖ ĒĢŁĒśłņĀäņĀ£ ļ░Å ļ╣äņŖżĒģīļĪ£ņØ┤ļō£ ņåīņŚ╝ņ¦äĒåĄņĀ£(nonsteroidal anti-inflammatory drug, NSAID) ņé¼ņÜ® ĒÖśņ×É ņłśņØś ņ”ØĻ░ĆņÖĆ ņŚ░Ļ┤ĆņØ┤ ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż. ĒŖ╣Ē׳, ņØĖĻĄ¼ Ļ│ĀļĀ╣ĒÖöņŚÉ ļö░ļØ╝ ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł ļ░£ņāØĻ│╝ Ļ┤ĆļĀ©ļÉ£ ĒĢŁĒśłņĀäņĀ£, NSAIDņØś ņ¦ĆņåŹņĀüņØĖ ļ│ĄņÜ®ņØĆ ņĢ×ņ£╝ļĪ£ļÅä ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£ĒśłņØ┤ ņ¦ĆņåŹņĀüņ£╝ļĪ£ ļ¼ĖņĀ£Ļ░Ć ļÉĀ ņłś ņ׳ņØīņØä ņŗ£ņé¼ĒĢ£ļŗż[5].
ĻĄŁļé┤ņÖĖ ļ¦ÄņØĆ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ NVUGIBļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉņØś ņ╣śļŻīņŚÉ ņ׳ņ¢┤ ļŗ©ņØ╝ ņ╣śļŻī ņĀäļץļ│┤ļŗżļŖö ĒÖśņ×ÉņØś Ļ░£ļ│äņĀüņØĖ ņ¦łļ│æ ņāüĒā£ņÖĆ ņāüĒÖ®, ĻĘĖļ”¼Ļ│Ā ņØśļŻīņ¦äņØś ņ×ÉņøÉ ļ░Å Ļ▓ĮĒŚśņØä Ļ│ĀļĀżĒĢ£ ļ¦×ņČżĒśĢ ņ╣śļŻīļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[9].
ļ│Ė ļĪĀ
ļé┤ņŗ£Ļ▓Į ņĀä Ļ┤Ćļ”¼(pre-endoscopy management)
ņ£äĒŚśļÅä ĒÅēĻ░Ć(risk stratification)
NVUGIB ĒÖśņ×ÉĻ░Ć ļé┤ņøÉĒĢ£ Ļ▓ĮņÜ░ ĒĢ┤ņÖĖ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ Glasgow Blatchford Score (GBS)ļź╝ ņØ┤ņÜ®ĒĢ£ ņ£äĒŚś ļČäļźśļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīņןĒĢ£ļŗż[11]. GBSļŖö ņłśĒśłņØ┤ļéś ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀĻ│╝ Ļ░ÖņØĆ ņżæņ×¼Ļ░Ć ĒĢäņÜöĒĢśņ¦Ć ņĢŖņØĆ ļé«ņØĆ ņ£äĒŚś ĒÖśņ×Éļź╝ ņŗØļ│äĒĢśļŖö ļŹ░ ļÅäņøĆņØ┤ ļÉśļ®░, ņĀÉņłśĻ░Ć 0 ļśÉļŖö 1ņØĖ ĒÖśņ×ÉļŖö ņ×ģņøÉ ņŚåņØ┤ ņÖĖļלņŚÉņä£ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢ£ļŗż[11]. ĻĄŁļé┤ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö GBSņÖĆ Ļ░ÖņØ┤ ņ£äĒŚśļÅäļź╝ ĒÅēĻ░ĆĒĢśļŖö ņ¦ĆĒæ£ļź╝ ĒÖ£ņÜ®ĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī ĒĢ┤ņÖĖ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņ▓śļ¤╝ ĻĄ¼ņ▓┤ņĀüņ£╝ļĪ£ ņ¦ĆĒæ£ņØś ņĀÉņłśņŚÉ ļö░ļØ╝ņä£ ĒÖśņ×Éļź╝ ņ¦äļŻīĒĢśļŖö ļé┤ņÜ®ņØĆ ĻĖ░ņłĀļÉśņ¢┤ ņ׳ņ¦Ć ņĢŖļŗż. ņØ┤ļŖö ĻĄŁļé┤ņØś ņØśļŻī ņĀæĻĘ╝ņä▒ ļ░Å ļé┤ņŗ£Ļ▓Į ņłśĻ░Ć ļō▒ņØä Ļ│ĀļĀżĒĢ£ Ļ▓░ņĀĢņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. GBSļŖö ļé«ņØĆ ņ£äĒŚś ĒÖśņ×Éļź╝ ļ¦żņÜ░ ļåÆņØĆ ļ»╝Ļ░ÉļÅäļĪ£ ņŗØļ│äĒĢĀ ņłś ņ׳ņ¦Ćļ¦ī, ņ¦æņżæ ņ╣śļŻīĻ░Ć ĒĢäņÜöĒĢ£ Ļ│Āņ£äĒŚś ĒÖśņ×Éļź╝ ņĀĢĒÖĢĒĢśĻ▓ī ņŗØļ│äĒĢśņ¦Ć ļ¬╗ĒĢśņŚ¼ ļ¦ÄņØĆ Ļ▓ĮņÜ░ņŚÉ ņ×äņāüņĀü ĒīÉļŗ©ņØ┤ ļŹö ņżæņÜöĒĢśļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£, Ļ│ĀļĀ╣, ļÅÖļ░ś ņŗ¼ļćīĒśłĻ┤Ć ņ¦łĒÖśņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░, ļīĆļ¤ē ĒåĀĒśł, ļé«ņØĆ ĒśłņĢĢ, ļ╣ĀļźĖ ļ¦źļ░Ģ ļō▒ņØś ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņĀüĻĘ╣ņĀüņØĖ ņåīņāØņłĀĻ│╝ ņżæĒÖśņ×Éņŗż ņ╣śļŻīļź╝ Ļ│ĀļĀżĒĢ┤ņĢ╝ ĒĢ£ļŗż.
PPI ņĀĢļ¦ź Ēł¼ņŚ¼
NVUGIBļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉņŚÉņä£ ņČ£Ēśł ļ│æņåīņØś ĒÖĢņØĖ ņŚåņØ┤ ļé┤ņŗ£Ļ▓Į ņŗ£Ē¢ē ņĀäņŚÉ PPIļź╝ ņĀĢļ¦źņ£╝ļĪ£ Ēł¼ņŚ¼ĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć ĒØöĒĢśļŗż. ņØ┤ļŖö PPIĻ░Ć ņČ£Ēśł ļ│æņåīņØś ņ¦ĆĒśłņŚÉ ĻĖ░ņŚ¼ĒĢśĻ│Ā ĒÖśņ×ÉņØś ņ×äņāüņĀü Ļ▓░Ļ│╝ņŚÉ ĻĖŹņĀĢņĀüņØĖ ņśüĒ¢źņØä ļ»Ėņ╣Ā Ļ▓āņ£╝ļĪ£ ņśłņāüļÉśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. ĻĘĖļ¤¼ļéś Ēśäņ×¼ ļŗżņ¢æĒĢ£ ņ¦äļŻī ņ¦Ćņ╣©ņŚÉņä£ļŖö ļé┤ņŗ£Ļ▓Į ņŗ£Ē¢ē ņĀä PPIņØś ņé¼ņÜ® ņŚ¼ļČĆņŚÉ ļīĆĒĢ┤ ļģ╝ļ×ĆņØ┤ ņ¦ĆņåŹļÉśĻ│Ā ņ׳ļŗż. Lau ļō▒[14]ņØ┤ ņŗ£Ē¢ēĒĢ£ ņ┤łĻĖ░ņØś ļ¼┤ņ×æņ£ä ļīĆņĪ░ ņŚ░ĻĄ¼(randomized controlled trial, RCT)ņŚÉņä£, PPI ņé¼ņÜ®ĻĄ░ņØĆ ļ╣äņé¼ņÜ®ĻĄ░ņŚÉ ļ╣äĒĢ┤ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒ¢łņØä ļĢī Ļ│Āņ£äĒŚś ņåīĻ▓¼ ļ░Å ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØś ĒĢäņÜöņä▒ņØ┤ ļé«ņØīņØä ļ│┤Ļ│ĀĒ¢łļŗż. ņØ┤ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ļ░öĒāĢņ£╝ļĪ£ ĻĄŁļé┤ ļ░Å ņ£Āļ¤ĮņØś ņ×äņāü Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ļé┤ņŗ£Ļ▓Į ņĀäņŚÉ ņĀĢļ¦ź ļé┤ PPI Ēł¼ņŚ¼ļź╝ Ļ▓āņØä ĻČīņןĒĢśĻ│Ā ņ׳ļŗż[10,12]. ĻĘĖļ¤¼ļéś ļ»ĖĻĄŁņØś ņ×äņāü Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ļé┤ņŗ£Ļ▓Į ņĀä PPI ņé¼ņÜ®ņŚÉ ļīĆĒĢ£ ļ¬ģĒÖĢĒĢ£ ĻČīĻ│Āļź╝ ņĀ£ņŗ£ĒĢśņ¦Ć ņĢŖĻ│Ā ņ׳ņ£╝ļ®░ ņśüĻĄŁ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ļé┤ņŗ£Ļ▓Į ņĀä PPIņØś ņé¼ņÜ®ņŚÉ ļ░śļīĆĒĢśļŖö ņ×ģņןņØä ņĘ©ĒĢśĻ│Ā ņ׳ļŗż[11,15]. ņØ┤ļ¤¼ĒĢ£ ĻĄŁņĀ£ņĀüņØĖ ņ¦Ćņ╣© ņ░©ņØ┤ļŖö Lau ļō▒[14]ņØś ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ņŚÉņä£ PPI ņé¼ņÜ®ņØ┤ ņé¼ļ¦ØļźĀ, ņ×¼ņČ£ĒśłļźĀ, ņłśņłĀņĀü ņ╣śļŻīņ£©ņŚÉ ļīĆĒĢ┤ ņ£ĀņØśĒĢ£ Ļ░£ņäĀņØä ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśĻĖ░ ļĢīļ¼Ėņ£╝ļĪ£ ĒĢ┤ņäØļÉĀ ņłś ņ׳ļŗż.
NVUGIBĻ░Ć ņØśņŗ¼ļÉśļŖö ĒÖśņ×ÉņŚÉĻ▓ī ļé┤ņŗ£Ļ▓Į ņĀä PPIļź╝ Ēł¼ņŚ¼ĒĢśļŖö Ļ▓āņØ┤ ļ╣äņÜ® ĒÜ©Ļ│╝ņĀüņØ┤ļØ╝ļŖö ļ│┤Ļ│ĀļÅä ņ׳ļŗż[16]. ļö░ļØ╝ņä£ ļ¬©ļōĀ ĒÖśņ×ÉņŚÉĻ▓ī ņØ╝Ļ┤äņĀüņ£╝ļĪ£ ļé┤ņŗ£Ļ▓Į ņĀä PPIļź╝ Ēł¼ņŚ¼ĒĢśĻĖ░ļ│┤ļŗżļŖö Ļ│Āņ£äĒŚśĻĄ░ņŚÉņä£ ņäĀĒāØņĀüņ£╝ļĪ£ Ēł¼ņŚ¼ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ņ£╝ļ®░, ļé┤ņŗ£Ļ▓Į ļ░Å ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØ┤ 24ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņØ┤ņÜ® Ļ░ĆļŖźĒĢśņ¦Ć ņĢŖĻ▒░ļéś ņāØļ¬ģņØä ņ£äĒśæĒĢśļŖö ņČ£ĒśłņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉļŖö ņĀĢļ¦ź ļé┤ PPIĻ░Ć ļÅäņøĆņØ┤ ļÉĀ ņłś ņ׳ļŗż.
ņ£äņןĻ┤ĆņÜ┤ļÅÖ ņ┤ēņ¦äņĀ£(prokinetics)
ļé┤ņŗ£Ļ▓Į ņżæ ņĀĢĒÖĢĒĢ£ ņ£äņןĻ┤Ć Ļ┤Ćņ░░Ļ│╝ ņĀüņĀłĒĢ£ ņ╣śļŻīļź╝ ņ£äĒĢ┤ņä£ļŖö ņŗ£ņĢ╝Ļ░Ć ņל ĒÖĢļ│┤ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż. NVUGIBļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉņŚÉņä£ļŖö ņ£ä ļśÉļŖö ņŗŁņØ┤ņ¦Ćņן ļé┤ņØś ĒśłņĀäņØ┤ļéś ņ×öņŚ¼ ņØīņŗØļ¼╝ļĪ£ ņØĖĒĢ┤ ņŗ£ņĢ╝ ĒÖĢļ│┤Ļ░Ć ņ¢┤ļĀżņÜĖ ņłś ņ׳ņ£╝ļ®░ ņØ┤ļŖö ļé┤ņŗ£Ļ▓ĮņĀü ņ╣śļŻīņØś ņä▒Ļ│ĄļźĀĻ│╝ ņ×¼ņČ£ĒśłļźĀņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣£ļŗż. ļ¦ÄņØĆ ņŚ░ĻĄ¼ņŚÉņä£ ĻĖēņä▒ ņāüļČĆ ņ£äņןĻ┤Ć ņČ£Ēśł ĒÖśņ×ÉņŚÉņä£ ļé┤ņŗ£Ļ▓Į ņĀä ņ£äņןĻ┤ĆņÜ┤ļÅÖ ņ┤ēņ¦äņĀ£ļĪ£ņä£ ņĀĢļ¦ź ļé┤ erythromycinņØś ĒÜ©ņÜ®ņä▒ņØ┤ ņ×ģņ”ØļÉ£ ļ░ö ņ׳ļŗż[17,18]. ĻĄŁļé┤ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ņ£äņןĻ┤ĆņÜ┤ļÅÖ ņ┤ēņ¦äņĀ£ņŚÉ ļīĆĒĢ£ ņ¢ĖĻĖēņØ┤ ņŚåņ£╝ļéś, ĒĢ┤ņÖĖĻ░Ć ņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ļé┤ņŗ£Ļ▓Į ņżæ ņŗ£ņĢ╝ Ļ░£ņäĀĻ│╝ ņ×¼ļé┤ņŗ£Ļ▓Į ĒĢäņÜöņä▒ņØś Ļ░Éņåīļź╝ ņ£äĒĢ┤ ņŗ£ņłĀ ņĀä ņĀĢļ¦ź ļé┤ erythromycinņØś ņé¼ņÜ®ņØä ĻČīņןĒĢśĻ│Ā ņ׳ļŗż[11]. ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£ļÅä ļé┤ņŗ£Ļ▓Į ņŗ£Ē¢ē ņĀä erythromycinņØś Ēł¼ņĢĮņØ┤ ļé┤ņŗ£Ļ▓Į ņŗ£ņĢ╝ņØś ņ¦łņØä Ē¢źņāüņŗ£ĒéżĻ│Ā, ņłśĒśłĻ│╝ ļ░śļ│Ą ļé┤ņŗ£Ļ▓ĮņØś ĒĢäņÜöņä▒, ļ│æņøÉ ņ×ģņøÉ ĻĖ░Ļ░äņØä ļŗ©ņČĢņŗ£ĒéżļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆļŗż[19]. ĻĘĖļ¤¼ļéś erythromycin ņĀĢļ¦źņĀ£ņĀ£ļŖö ĻĄŁļé┤ ļ░Å ņŚ¼ļ¤¼ ĻĄŁĻ░ĆņŚÉņä£ ņé¼ņÜ®ņØ┤ ņĀ£ĒĢ£ļÉśņ¢┤ ņ׳ļŗż. ErythromycinņØä ļīĆņŗĀĒĢśņŚ¼ ļé┤ņŗ£Ļ▓Į ņĀä metoclopramideņØś Ēł¼ņĢĮņØĆ ņĀäļ░śņĀüņØĖ ļé┤ņŗ£Ļ▓Į ņŗ£ņĢ╝ Ļ░£ņäĀņŚÉļŖö ĒÜ©Ļ│╝Ļ░Ć ņŚåņŚłņ£╝ļéś ņ£ä ĻĖ░ņĀĆļČĆņØś ņŗ£ņĢ╝ļź╝ Ļ░£ņäĀĒĢśĻ│Ā, ļ░śļ│Ą ļé┤ņŗ£Ļ▓ĮņØś ĒĢäņÜöņä▒ņØä ļé«ņČöļŖö Ļ▓āņ£╝ļĪ£ ņĄ£ĻĘ╝ ļ│┤Ļ│ĀļÉśņŚłļŗż[20].
ErythromycinņØĆ ņĀĢļ¦ź ļé┤ļĪ£ 250 mgņØä 20ļČäņŚÉņä£ 30ļČä Ļ░ä Ēł¼ņŚ¼ĒĢśļŖö Ļ▓āņØ┤ ĻČīņןļÉśĻ│Ā, Ēł¼ņĢĮ ņÖäļŻī Ēøä 20ļČäņŚÉņä£ 90ļČä ņé¼ņØ┤ņŚÉ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ļ░öļ×īņ¦üĒĢśļŗż[17,18]. ErythromycinņØä Ēł¼ņŚ¼ ļ░øļŖö ĒÖśņ×ÉļŖö QT Ļ░äĻ▓® ņŚ░ņן ņŚ¼ļČĆļź╝ ņŻ╝ņØś Ļ╣ŖĻ▓ī ļ¬©ļŗłĒä░ļ¦üĒĢĀ ĒĢäņÜöĻ░Ć ņ׳ļŗż. ļśÉĒĢ£ erythromycinņØĆ cytochrome P450 3A ņ¢ĄņĀ£ņĀ£ņØ┤ļ»ĆļĪ£ Ēł¼ņŚ¼ ņĀäņŚÉ ņāüĒśĖņ×æņÜ®ņØä ĒĢśļŖö ņĢĮņĀ£Ļ░Ć ņ׳ļŖöņ¦Ć ĒÖĢņØĖĒĢ┤ņĢ╝ ĒĢ£ļŗż[18,21-24]. MetoclopramideļŖö 10 mgņØś ņÜ®ļ¤ēņØä 10 mLņØś ņāØļ”¼ņŗØņŚ╝ņłśņÖĆ Ēś╝ĒĢ®ĒĢśņŚ¼ 5ļČäĻ░ä ņŻ╝ņé¼ĒĢśļ®░ Ēł¼ņĢĮ ņÖäļŻī Ēøä 30ļČäņŚÉņä£ 120ļČä ņé¼ņØ┤ņŚÉ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ĻČīĻ│ĀļÉ£ļŗż[20,25].
ļé┤ņŗ£Ļ▓Į ņ╣śļŻī(endoscopic treatment)
ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ ņŗ£ĻĖ░
NVUGIB ĒÖśņ×ÉĻ░Ć ņØæĻĖēņŗżņŚÉ ļé┤ņøÉĒ¢łņØä ļĢī ņ¢ĖņĀ£ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢĀ Ļ▓āņØĖņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ļģ╝ļ×ĆņØ┤ ņ׳ņŚłļŗż. ņØ╝ļ░śņĀüņ£╝ļĪ£ urgent endoscopyļŖö ļé┤ņøÉ Ēøä 12ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØä ņØśļ»ĖĒĢśļ®░ early endoscopyļŖö 24ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØä ņØśļ»ĖĒĢ£ļŗż[12]. ļ╣ĀļźĖ ņŗ£Ļ░ä ļé┤ņŚÉ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļ®┤ ĒÖśņ×ÉņØś ņ×äņāü Ļ▓ĮĻ│╝Ļ░Ć Ļ░£ņäĀļÉĀ Ļ▓āņ£╝ļĪ£ ņśłņāüļÉśņŚłņ£╝ļéś ļŹ┤ļ¦łĒü¼ņŚÉņä£ ņ¦äĒ¢ēļÉ£ ļīĆĻĘ£ļ¬© ņĀäĻĄŁ ņĮöĒśĖĒŖĖ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤ urgent endoscopyļź╝ ļ░øļŖö ĒÖśņ×ÉņŚÉņä£ ņé¼ļ¦ØļźĀņØ┤ ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[26]. ņĄ£ĻĘ╝ GBS ņĀÉņłśĻ░Ć 12ņĀÉ ņØ┤ņāüņØĖ Ļ│Āņ£äĒŚś ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ĒÖŹņĮ®ņŚÉņä£ ņŗ£Ē¢ēĒĢ£ RCT ņŚ░ĻĄ¼ņŚÉņä£ NVUGIB ĒÖśņ×Éļź╝ urgent endoscopy (6ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņŗ£Ē¢ē)ļź╝ ņŗ£Ē¢ēĒĢ£ ĻĄ░Ļ│╝ early endoscopy (24ņŗ£Ļ░ä ņØ┤ļé┤)ļź╝ ņŗ£Ē¢ēĒĢ£ ĻĄ░ņ£╝ļĪ£ ļ╣äĻĄÉĒ¢łņØä ļĢī, 30ņØ╝ ņé¼ļ¦ØļźĀ, ņČöĻ░Ć ņČ£Ēśł, ņ×ģņøÉ ĻĖ░Ļ░ä, ņłśĒśł ĒĢäņÜöņä▒ņŚÉņä£ ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż[27]. ņ£Āļ¤Į Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ĒÖśņ×ÉņØś ņ×äņāü Ļ▓░Ļ│╝ņŚÉ Ēü░ ņØ┤ļōØņØ┤ ņŚåĻĖ░ņŚÉ 12ņŗ£Ļ░ä ņØ┤ļé┤ņØś ļé┤ņŗ£Ļ▓ĮņØä ĻČīņןĒĢśņ¦Ć ņĢŖņ£╝ļ®░, 6ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ņŗ£Ē¢ēĒĢśļŖö urgent endoscopyļŖö ĒÖśņ×ÉņØś ņ×äņāü Ļ▓░Ļ│╝ļź╝ ņĢģĒÖöņŗ£Ēé¼ ņłś ņ׳ļŗżĻ│Ā ņ¢ĖĻĖēĒĢśĻ│Ā ņ׳ļŗż[12]. ĻĄŁļé┤ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļÅä 24ņŗ£Ļ░ä ņØ┤ļé┤ņŚÉ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśļ®░ ņ×äņāüņØśņØś ĒīÉļŗ©ņŚÉ ļö░ļØ╝ ļé┤ņŗ£Ļ▓Į ņŗ£Ē¢ē ņŚ¼ļČĆļź╝ Ļ▓░ņĀĢĒĢśļÅäļĪØ ĻČīĻ│ĀĒĢ£ļŗż[10]. ĒĢ£ Ļ░Ćņ¦Ć ņŻ╝ņØśĒĢĀ ņĀÉņØĆ ĒÖŹņĮ®ņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņČ®ļČäĒĢ£ ņłśņĢĪņ╣śļŻīņŚÉļÅä ņĀĆĒśłņĢĢ ņć╝Ēü¼Ļ░Ć ņ¦ĆņåŹļÉ£ ĒÖśņ×ÉļōżņØ┤ ņĀ£ņÖĖļÉśņŚłļŗż. ņ”ē ņČ®ļČäĒĢ£ ņłśņĢĪņ╣śļŻīņŚÉļÅä ĒśłņŚŁĒĢÖņĀüņ£╝ļĪ£ ļČłņĢłņĀĢĒĢ£ ĒÖśņ×ÉņŚÉņä£ļŖö ņĪ░ĻĖ░ņŚÉ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØä Ļ│ĀļĀżĒĢ┤ ļ│┤ņĢäņĢ╝ ĒĢ£ļŗż.
ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀ(endoscopic therapeutic methods)
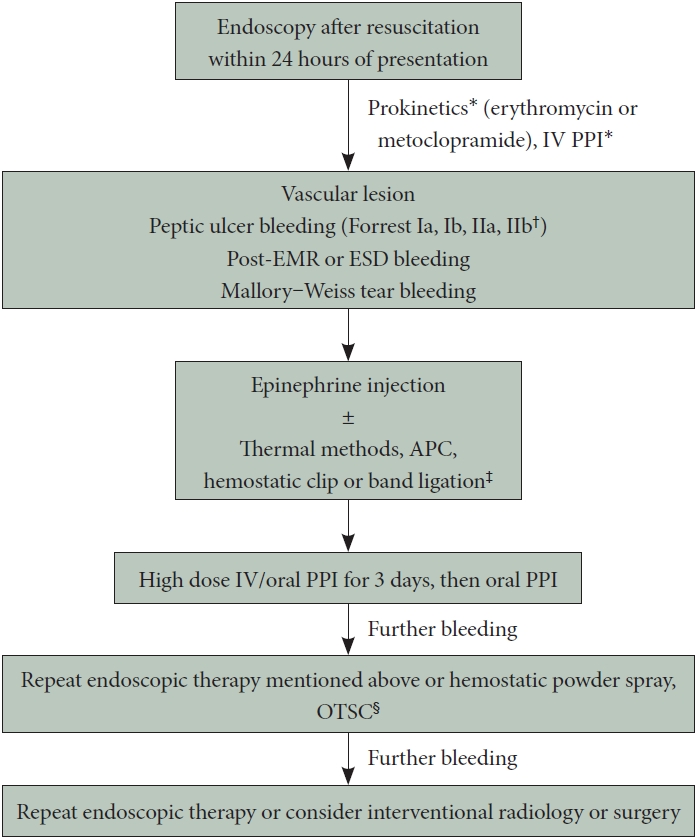
ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł ĒÖśņ×ÉņØś Ļ▓ĮņÜ░, ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ ņżæ Ļ┤Ćņ░░ļÉśļŖö Forrest ļČäļźśņŚÉ ļö░ļØ╝ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØś ņŗ£Ē¢ēņŚ¼ļČĆĻ░Ć Ļ▓░ņĀĢļÉ£ļŗż[10]. ĒÖ£ļÅÖņä▒ ņČ£Ēśł ņåīĻ▓¼(Forrest Ia, Ib)Ļ│╝ ļģĖņČ£ ĒśłĻ┤Ć(Forrest IIa)ņØä Ļ░Ćņ¦ä Ļ▓ĮņÜ░ļŖö Ļ│Āņ£äĒŚś ļ│æļ│Ćņ£╝ļĪ£ ņĀĢņØśļÉśļ®░, ņāēņåī ļ░śņĀÉ(Forrest IIc)ņØ┤ ņ׳Ļ▒░ļéś Ļ╣©ļüŚĒĢ£ ĻČżņ¢æ ĻĖ░ņĀĆ(Forrest III)ļŖö ņĀĆņ£äĒŚśĻĄ░ņ£╝ļĪ£ ļČäļźśļÉ£ļŗż. ĒśłņĀäņØ┤ ļČĆņ░®ļÉśņ¢┤ ņ׳ļŖö Forrest IIbļź╝ Ļ│Āņ£äĒŚśĻĄ░ņ£╝ļĪ£ ļČäļźśĒĢĀņ¦ĆņŚÉ ļīĆĒĢ┤ņä£ļŖö ļģ╝ļ×ĆņØ┤ ņ׳ņ£╝ļ®░, ņ£Āļ¤Į Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ĒĢ┤ļŗ╣ ļ│æņåīņØś ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØä ĻČīĻ│ĀĒĢśņ¦Ćļ¦ī ļ»ĖĻĄŁ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö Ļ░£ļ│ä ņŚ░ĻĄ¼ņØś ĻĘ£ļ¬©Ļ░Ć ņ×æĻ│Ā Ļ▓░Ļ│╝ņØś ņØ╝Ļ┤Ćņä▒ņØ┤ ļ¢©ņ¢┤ņ¦äļŗżĻ│Ā ĒīÉļŗ©ĒĢśņŚ¼ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØś ĒĢäņÜöņä▒ņŚÉ ļīĆĒĢ┤ ļ¬ģĒÖĢĒĢ£ ĻČīĻ│Āļź╝ ļé┤ļ”¼ņ¦Ć ņĢŖņĢśļŗż[11,12]. ņØ╝ļ░śņĀüņ£╝ļĪ£ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØĆ Ļ│Āņ£äĒŚś ļ│æļ│ĆņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉ ĒĢ£ĒĢśņŚ¼ ĻČīņןļÉ£ļŗż. ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØĆ injection therapy (ņśł: diluted epinephrine, sclerosant), contact or non-contact thermal methods (ņśł: monopolar or bipolar electrocoagulation, argon plasma coagulation [APC]), mechanical methods (ņśł: hemostatic clip, band ligation)ļĪ£ ĻĄ¼ļČäļÉ£ļŗż. Ļ░üĻ░üņØś ņ¦ĆĒśłņłĀņØś ĒÜ©ļŖźņØä ļ╣äĻĄÉĒĢ£ RCTĻ░Ć ļ¦Äņ¦Ć ņĢŖņĢä, ņĀüņĀłĒĢ£ ņ¦ĆĒśłņłĀņØś ņäĀĒāØņØĆ ņČ£Ēśł ļ│æļ│ĆņØś ņ£äņ╣śņÖĆ ĒśĢĒā£, ņøÉņØĖĻ│╝ ĒŖ╣ņä▒, ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļŖö ņØśņé¼ņÖĆ ļ│┤ņĪ░ņØĖļĀźņØś ņłÖļĀ©ļÅä ļ░Å ņäĀĒśĖļÅä, ĻĘĖļ”¼Ļ│Ā ĒŖ╣ņĀĢ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØś Ļ░ĆņÜ®ņä▒ņŚÉ ļö░ļØ╝ Ļ▓░ņĀĢļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż(Table 1) [9].
ņŻ╝ņé¼ ņ╣śļŻī(injection therapy)
ņŻ╝ņé¼ ņ╣śļŻīļŖö ņČ£Ēśł ļ│æņåīņŚÉ epinephrine, sclerosant (ņśł: ethanol, ethanolamine) ļ░Å tissue adhesive (ņśł: thrombin, cyanoacrylate)ļź╝ ņŻ╝ņ×ģĒĢśļŖö ļ░®ļ▓ĢņØ┤ļŗż. ņ×äņāüņŚÉņä£ļŖö ņŻ╝ļĪ£ epinephrineņØä ņāØļ”¼ņŗØņŚ╝ņłśņÖĆ Ēś╝ĒĢ®ĒĢ£ ĒؼņäØņĢĪ(1:10000 ļśÉļŖö 1:20000)ņØä ņé¼ņÜ®ĒĢśļ®░, ļ│æļ│ĆņØś ņŻ╝ņ£ä ņé¼ļ░®ņŚÉ 0.5 mLņŚÉņä£ 2 mLļź╝ ņŻ╝ņ×ģĒĢśņŚ¼ ņĪ░ņ¦üņØä ņĢĢļ░ĢĒĢśĻ│Ā ĒśłĻ┤Ć ņłśņČĢņØä ĒåĄĒĢ┤ ņ¦ĆĒśł ĒÜ©Ļ│╝ļź╝ ņĀ£Ļ│ĄĒĢ£ļŗż. ĻĘĖļ¤¼ļéś epinephrine ņŻ╝ņ×ģ ļŗ©ļÅģ ņÜöļ▓ĢņØĆ ļŗżļźĖ ņ¦ĆĒśłņłĀņŚÉ ļ╣äĒĢ┤ ĒÜ©Ļ│╝Ļ░Ć ņāüļīĆņĀüņ£╝ļĪ£ ļé«ņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ¢┤, ņŻ╝ļĪ£ ļŗżļźĖ ņ¦ĆĒśłņłĀĻ│╝ ļ│æĒĢ®ĒĢśņŚ¼ ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØä ĻČīņןĒĢ£ļŗż[11,28]. ņŻ╝ņé¼ ņÜöļ▓ĢņØś ņןņĀÉņØĆ Ēł¼ņŚ¼Ļ░Ć ņēĮĻ│Ā, ĒÖ£ļÅÖņä▒ ņČ£ĒśłņØ┤ Ļ┤Ćņ░░ļÉĀ ļĢī ņČ£ĒśłņØä ņØ╝ņŗ£ņĀüņ£╝ļĪ£ ņżäņŚ¼ ļé┤ņŗ£Ļ▓Į ņŗ£ņĢ╝ļź╝ ĒÖĢļ│┤ĒĢ©ņ£╝ļĪ£ņŹ© ļ│┤ļŗż ĒÖĢņŗżĒĢ£ ļé┤ņŗ£Ļ▓Į ņ╣śļŻīļ▓Ģ(ņśł: hemostatic clip or thermal methods)ņØä ņÜ®ņØ┤ĒĢśĻ▓ī ĒĢ┤ņżĆļŗż.
ņ¦ĆĒśł Ēü┤ļ”Į(hemostatic clip)
ņ¦ĆĒśł Ēü┤ļ”ĮņØĆ ņØ╝ļ░śņĀüņ£╝ļĪ£ ņČ£Ēśł ļČĆņ£äņŚÉ ĻĖ░Ļ│äņĀü ņĢĢļ░ĢņØä Ļ░ĆĒĢ┤ ņ¦ĆĒśłņØä ļŗ¼ņä▒ĒĢśļŖö ļ░®ļ▓ĢņØ┤ļŗż. ņØ┤ļŖö ņ×äņāüņŚÉņä£ ņ¦ĆĒśłņØä ņ£äĒĢ┤ Ļ░Ćņן ļäÉļ”¼ ņé¼ņÜ®ļÉśļŖö ļ░®ļ▓Ģ ņżæ ĒĢśļéśņØ┤ņ¦Ćļ¦ī ņŗżņĀ£ ņØ┤ņØś ĒÜ©Ļ│╝ņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļŖö ņĀ£ĒĢ£ņĀüņØ┤ļŗż[28-30]. ņ¦ĆĒśł Ēü┤ļ”ĮņØĆ ņåīĒÖöņä▒ ĻČżņ¢æļ┐Éļ¦ī ņĢäļŗłļØ╝ Dieulafoy ļ│æļ│ĆĻ│╝ Ļ░ÖņØĆ ĒśłĻ┤Ćņä▒ ļ│æļ│ĆņŚÉļÅä ņé¼ņÜ®ļÉĀ ņłś ņ׳ļŗż[31,32]. ĻĘĖļ¤¼ļéś ņ£äņØś ļČäļ¼ĖļČĆņÖĆ Ļ░ÖņØĆ ĒŖ╣ņĀĢ ņ£äņ╣ś Ēś╣ņØĆ ņä¼ņ£ĀĒÖöļÉ£ ĻČżņ¢æ ĻĖ░ņĀĆļČĆ ļō▒ņŚÉņä£ļŖö ĻĖ░ņłĀņĀüņ£╝ļĪ£ ņé¼ņÜ®ņØ┤ ņ¢┤ļĀĄļŗżļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŗż. ņĄ£ĻĘ╝ņŚÉļŖö over-the-scope-clip (OTSC)ņØ┤ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀļĪ£ ņČöņ▓£ļÉśĻ│Ā ņ׳ļŗż. OTSCļŖö Ļ│Āņ£äĒŚś ĒÖśņ×ÉņŚÉņä£ ĻĖ░ņĪ┤ņØś Ēü┤ļ”ĮņŚÉ ļ╣äĒĢ┤ ņ×¼ņČ£Ēśł Ļ░ÉņåīņŚÉ ļŹö ĒÜ©Ļ│╝ņĀüņØĖ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[33]. ļ»ĖĻĄŁ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ņØ╝ņ░© ņ¦ĆĒśłņłĀņŚÉļÅä ņČ£ĒśłņØ┤ ņ¦ĆņåŹļÉśĻ▒░ļéś ņ×¼ļ░£ĒĢśļŖö Ļ▓ĮņÜ░ ĻĄ¼ņĪ░ņÜöļ▓Ģņ£╝ļĪ£ OTSCļź╝ ņé¼ņÜ®ĒĢĀ Ļ▓āņØä ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[11]. ĻĘĖļ¤¼ļéś ĻĄŁļé┤ņŚÉņä£ļŖö ņČ£Ēśł ĒÖśņ×ÉņŚÉņä£ņØś OTSC ņé¼ņÜ®ņØ┤ Ļ▒┤Ļ░Ģļ│┤ĒŚśĻĖēņŚ¼ ļīĆņāüņ£╝ļĪ£ ņØĖņĀĢļÉśņ¦Ć ņĢŖņĢä, ņŗżņĀ£ ņ×äņāü ĒÖśĻ▓ĮņŚÉņä£ ļ╣äņÜ® ļīĆļ╣ä ĒÜ©Ļ│╝Ļ░Ć ļ¢©ņ¢┤ņ¦äļŗżļŖö ļ¼ĖņĀ£Ļ░Ć ņ׳ļŗż.
ņĀæņ┤ē ņŚ┤ņ╣śļŻī(contact thermal methods)
ņĀæņ┤ē ņŚ┤ņ╣śļŻīļŖö ņŚ┤ņØä ņāØņä▒ĒĢśņŚ¼ ņĪ░ņ¦üņØś ņØæĻ│ĀņÖĆ ĒśłĻ┤ĆņØś ņłśņČĢņ£╝ļĪ£ ņ¦ĆĒśłņØä ļŗ¼ņä▒ĒĢśļŖö ļ░®ļ▓ĢņØ┤ļŗż. ĒĢ┤ņÖĖ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö bipolar electrocoagulation, heater probe ļ░Å monopolar soft coagulationņØä ņåīĻ░£ĒĢśņ¦Ćļ¦ī ņŗżņĀ£ ĻĄŁļé┤ņŚÉņä£ļŖö hemostatic forcep (ņśł: CoagrasperŌäó; Olympus, Tokyo, Japan)ņØä ņØ┤ņÜ®ĒĢ£ electrocoagulationņØ┤ Ļ░Ćņן ļ¦ÄņØ┤ ņé¼ņÜ®ļÉ£ļŗż. ņĄ£ĻĘ╝ ļ░£Ēæ£ļÉ£ RCT ņŚ░ĻĄ¼ņŚÉ ņØśĒĢśļ®┤ hemostatic forcepņØĆ hemostatic clipņŚÉ ļ╣äĒĢ┤ ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł ņ╣śļŻīņŚÉņä£ ņ┤łĻĖ░ ņ¦ĆĒśł ņä▒Ļ│ĄļźĀņØ┤ ļŹö ļåÆĻ│Ā ņ×¼ņČ£ĒśłļźĀņØ┤ ļé«ņØĆ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[34].
ļ╣äņĀæņ┤ē ņŚ┤ņ╣śļŻī(non-contact thermal methods)
ļ╣äņĀæņ┤ē ņŚ┤ņ╣śļŻīņŚÉļŖö APCĻ░Ć Ļ░Ćņן ļīĆĒæ£ņĀüņØ┤ļŗż. APCļŖö ņŻ╝ļĪ£ ĒśłĻ┤ĆņØ┤ĒśĢņä▒ņ”Ø ļ░Å gastric antral vascular ectasia (GAVE)ņÖĆ Ļ░ÖņØĆ Ēæ£ļ®┤ ĒśłĻ┤Ć ļ│æļ│ĆņØś ņ¦ĆĒśłņŚÉ ņé¼ņÜ®ļÉ£ļŗż[35,36]. Heater probe Ēś╣ņØĆ hemostatic clipĻ│╝ ļ╣äĻĄÉĒ¢łņØä ļĢī, APCĻ░Ć ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£ĒśłņØä ļŗżļŻ©ļŖö ļŹ░ ņ׳ņ¢┤ņä£ ļŹö ĒÜ©Ļ│╝ņĀüņØ╝ ņłś ņ׳ļŗżļŖö ņŚ░ĻĄ¼ Ļ▓░Ļ│╝Ļ░Ć ņ׳ļŗż[37]. ĻĘĖļ¤¼ļéś ļ»ĖĻĄŁ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł ĒÖśņ×ÉņØś ņ¦ĆĒśłņŚÉ APCņØś ņé¼ņÜ®ņŚÉ ļīĆĒĢ£ ĻĘ╝Ļ▒░Ļ░Ć ļŗżļźĖ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀļ│┤ļŗż ļŹö ņĀüļŗżļŖö ņØ┤ņ£ĀļĪ£ ņĪ░Ļ▒┤ļČĆļĪ£ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[11].
ņ¦ĆĒśł ņŖżĒöäļĀłņØ┤(hemostatic powder spray)
ņĄ£ĻĘ╝ NVUGIB ļČäņĢ╝ņŚÉņä£ ņŻ╝ļ¬®ĒĢĀ ļ¦īĒĢ£ ļ░£ņĀä ņżæ ĒĢśļéśļŖö ĻĄŁņåī ņ¦ĆĒśłņĀ£ņØś ļÅäņ×ģņØ┤ļŗż. ņØ┤ļōżņØĆ ļ╣äņĀæņ┤ē ļ░®ņŗØņ£╝ļĪ£ ņ¦ĆĒśł ĒÜ©Ļ│╝ļź╝ ļ░£Ē£śĒĢśļ®░, ļŗżļźĖ ņ¦ĆĒśłņłĀņŚÉ ļ╣äĒĢ┤ ļäōņØĆ ņČ£Ēśł ņśüņŚŁņŚÉ ņĀüņÜ® Ļ░ĆļŖźĒĢśĻ│Ā ĻĖ░ņłĀņĀüņ£╝ļĪ£ ņĀüņÜ®ņØ┤ ņēĮļŗżļŖö ņןņĀÉņØ┤ ņ׳ļŗż. ĒŖ╣Ē׳, ņĢģņä▒ ņóģņ¢æĻ│╝ Ļ░ÖņØ┤ ļäōĻ▓ī ņČ£ĒśłĒĢśļŖö ļ│æļ│ĆņŚÉ ĒÜ©Ļ│╝ņĀüņØ┤ļŗż[38,39].
Ēśäņ×¼Ļ╣īņ¦Ć Ļ░£ļ░£ļÉ£ 5Ļ░£ņØś ņĀ£ĒÆł ņżæ ĻĄŁļé┤ņŚÉņä£ļŖö 3Ļ░Ćņ¦ĆĻ░Ć ņé¼ņÜ® Ļ░ĆļŖźĒĢśļ®░(Table 2), Ļ░Ćņן ļäÉļ”¼ ņŚ░ĻĄ¼ļÉ£ ņĀ£ĒÆłņØĆ TC-325 (Hemospray Ōäó; Cook Medical, Bloomington, IN, USA)ņØ┤ļŗż. ņØ┤ņÖĖņŚÉļÅä ĻĄŁļé┤ Ļ░£ļ░£ ņĀ£ĒÆłņØĖ NexpowderŌäó, CGBioŌäóņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļōżļÅä ļ░£Ēæ£ļÉśĻ│Ā ņ׳ļŗż[40-42]. ļīĆļČĆļČäņØś ņŚ░ĻĄ¼ņŚÉņä£ ņÜ░ņłśĒĢ£ ņ┤łĻĖ░ ņ¦ĆĒśłļźĀņØä ļ│┤ņŚ¼ņŻ╝ņŚłņ£╝ļéś, ļÅäĒż Ēøä 12-24ņŗ£Ļ░ä ņØ┤ĒøäņŚÉļŖö ļČäļ¦ÉņØ┤ ņö╗Ļ▓© ļéśĻ░Ćļ®┤ņä£ ņ×¼ņČ£ĒśłņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗżļŖö ņÜ░ļĀżĻ░Ć ņ׳ļŗż[43,44]. ņ£Āļ¤Į Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ņ×¼ņČ£ĒśłņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ņŚÉ ņ¦ĆĒśł ņŖżĒöäļĀłņØ┤ņØś ņé¼ņÜ®ņØä ņĀ£ņĢłĒĢśļ®░ ļ»ĖĻĄŁ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ĒÖ£ļÅÖņä▒ ņČ£ĒśłņØ┤ ņ׳ļŖö ĒÖśņ×ÉņŚÉĻ▓ī ņ┤łņ╣śļŻīņØś ņäĀĒāØņ¦Ć ņżæ ĒĢśļéśļĪ£ ĻČīĻ│ĀĒĢśĻ│Ā ņ׳ļŗż[11,12].
ļé┤ņŗ£Ļ▓Į Ēøä Ļ┤Ćļ”¼(post-endoscopic management)
ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼(second-look endoscopy)
ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļŖö ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀ ņŗ£Ē¢ē Ēøä 1-2ņØ╝ ņØ┤ļé┤ņŚÉ ņ×¼ņČ£Ēśł ņåīĻ▓¼ņØ┤ ņŚåņØä ļĢī ņŗ£Ē¢ēĒĢśļŖö ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļĪ£ ņĀĢņØśļÉ£ļŗż[10]. ņØ┤ Ļ▓Ćņé¼ļŖö ņ×¼ņČ£Ēśł ņ£äĒŚśņØä ļé«ņČöĻ│Ā ņØæĻĖēņłśņłĀņØś ĒĢäņÜöņä▒ņØä ņżäņØ┤ĻĖ░ ņ£äĒĢ┤ ņŗ£Ē¢ēļÉ£ļŗż. ĻĘĖļ¤¼ļéś ĻĄŁļé┤ ņŚ░ĻĄ¼ņŚÉ ļö░ļź┤ļ®┤, ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓ĮņØ┤ ļŗ©ņØ╝ ļé┤ņŗ£Ļ▓ĮņŚÉ ļ╣äĒĢ┤ ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł ĒÖśņ×ÉņŚÉņä£ ņ×ģņøÉ ĻĖ░Ļ░ä, ņłśĒśłļ¤ē, ņé¼ļ¦ØļźĀņŚÉ ļŹö ņÜ░ņłśĒĢśņ¦Ć ņĢŖņØĆ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[45]. ļśÉĒĢ£ 9Ļ░£ņØś RCTļź╝ ĒżĒĢ©ĒĢ£ ļ®öĒāĆļČäņäØ ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓ĮņØ┤ ļŗ©ņØ╝ ļé┤ņŗ£Ļ▓ĮņŚÉ ļ╣äĒĢ┤ ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł ĒÖśņ×ÉņØś ņ×¼ņČ£Ēśł, ņé¼ļ¦ØļźĀ, ņłśņłĀļźĀ Ļ░ÉņåīņŚÉ ņ׳ņ¢┤ ņÜ░ņłśĒĢśņ¦Ć ņĢŖņĢśļŗż[46]. ĒĢ┤ņÖĖ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņØĆ ņ×¼ņČ£ĒśłņØś ņ×äņāüņĀü ņ”ØĻ▒░Ļ░Ć ņŚåļŖö Ļ▓ĮņÜ░ ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓ĮņØä ĻČīĻ│ĀĒĢśņ¦Ć ņĢŖļŖöļŗż[12,13]. ļ░śļ®┤, ĻĄŁļé┤ Ļ░ĆņØ┤ļō£ļØ╝ņØĖņŚÉņä£ļŖö ņ×¼ņČ£ĒśłņØś ņ£äĒŚśņØ┤ ļåÆņØĆ Ļ▓ĮņÜ░ ņØ┤ņ░© ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗżĻ│Ā ĻČīĻ│ĀĒĢśļéś, ņ¢┤ļ¢ż ĒÖśņ×ÉņŚÉĻ▓ī ļÅäņøĆņØ┤ ļÉĀņ¦ĆņŚÉ ļīĆĒĢ£ ĻĄ¼ņ▓┤ņĀüņØĖ ņ¦Ćņ╣©ņØĆ ņĀ£ņŗ£ļÉśņ¦Ć ņĢŖņĢśļŗż[10].
ņĄ£ĻĘ╝ ĻĄŁļé┤ņŚÉņä£ 699ļ¬ģņØś ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ņ¦äĒ¢ēĒĢ£ ņĀäĒ¢źņĀü ņĮöĒśĖĒŖĖ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśł Ēøä ņ×¼ņČ£ĒśłņØś ņ£äĒŚś ņ”ØĻ░Ć ņÜöņåīļĪ£ NSAIDņØś ņé¼ņÜ®, ļīĆļ¤ē ņłśĒśł, ĻĘĖļ”¼Ļ│Ā ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓ĮņØś ņŗżĒī©Ļ░Ć ĒÖĢņØĖļÉśņŚłļŗż[47]. ļö░ļØ╝ņä£ ņ┤łĻĖ░ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņØ┤ ļČłņÖäņĀäĒĢ£ Ļ▓ĮņÜ░, NSAIDņØś ņé¼ņÜ®, ļīĆļ¤ē ņłśĒśł ĒÖśņ×ÉņŚÉĻ▓īņä£ ņØ┤ņ░© Ļ┤Ćņ░░ ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļŖö Ļ▓āņØ┤ ļÅäņøĆņØ┤ ļÉĀ ņłś ņ׳ļŗż[45].
ņé░ļČäļ╣ä ņ¢ĄņĀ£ ņÜöļ▓Ģ(acid suppression after endoscopy)
Ļ│Āņ£äĒŚś ņåīĒÖöņä▒ ĻČżņ¢æ ņČ£Ēśł(Forrest I, IIa ļ░Å IIb) ĒÖśņ×ÉņŚÉĻ▓īļŖö Ļ│ĀņÜ®ļ¤ē PPIļź╝ 3ņØ╝Ļ░ä Ēł¼ņŚ¼ĒĢ┤ņĢ╝ ĒĢ£ļŗż[48]. Ļ│ĀņÜ®ļ¤ē PPIļŖö ņĀĢļ¦ź ļé┤ 80 mgņØś ņ┤łĻĖ░ ļĪ£ļö® ņÜ®ļ¤ēņ£╝ļĪ£ ņŗ£ņ×æĒĢśļ®░, ņØ┤ņ¢┤ņä£ ņŗ£Ļ░äļŗ╣ 8 mgņØś ņ¦ĆņåŹņĀüņØĖ ņŻ╝ņ×ģ ļśÉļŖö Ļ░äĒŚÉņĀü ņŻ╝ņ×ģ(ņśł: ĒĢśļŻ©ņŚÉ ļæÉ ļ▓ł ļśÉļŖö ņäĖ ļ▓ł 4 0 m g)ņØä ņØśļ»ĖĒĢ£ļŗż. 3ņØ╝Ļ░äņØś Ēł¼ņŚ¼ Ēøä, 2ņŻ╝ ļÅÖņĢł ĒĢśļŻ© ļæÉ ļ▓ł Ļ▓ĮĻĄ¼ PPIļź╝ Ēł¼ņŚ¼ĒĢśĻ│Ā 2ņŻ╝ ĒøäņŚÉļŖö ĒĢśļŻ©ņŚÉ ĒĢ£ ļ▓ł ļ│ĄņÜ®ĒĢ£ļŗż. ņĀĆņ£äĒŚś ĒÖśņ×ÉļŖö Ļ│ĀņÜ®ļ¤ē PPIļź╝ ĒĢäņÜöļĪ£ ĒĢśņ¦Ć ņĢŖņ£╝ļ®░, ļ░öļĪ£ Ļ▓ĮĻĄ¼ PPIļź╝ ļ│ĄņÜ®ĒĢśĻ│Ā ņĀĢņāü ņŗØļŗ©ņ£╝ļĪ£ ļÅīņĢäĻ░ł ņłś ņ׳ļŗż.
PPIņÖĆ clopidogrel Ļ░äņØś ņ×Āņ×¼ņĀü ņāüĒśĖ ņ×æņÜ®ņŚÉ ļīĆĒĢ£ ņ┤łĻĖ░ ņÜ░ļĀżĻ░Ć ņĀ£ĻĖ░ļÉśņŚłņ£╝ļéś ņ×äņāüņĀüņ£╝ļĪ£ Ļ┤ĆļĀ©ņä▒ņØ┤ ņ×ģņ”ØļÉśņ¦Ć ņĢŖņĢśļŗż[13]. ņĢäņŖżĒö╝ļ”░, NSAID ļ░Å ļ╣äņäĀĒāØņĀü cyclooxygenase-2 (COX-2)ņ¢ĄņĀ£ņĀ£, ĒĢŁņØæĻ│ĀņĀ£ļź╝ ĒĢäņÜöļĪ£ ĒĢśļŖö ĒÖśņ×É ļ░Å ņåīĒÖöņä▒ ĻČżņ¢æ ņ¦łĒÖśņØś ņøÉņØĖņØä ņ░ŠņØä ņłś ņŚåļŖö ĒÖśņ×É(ņ”ē, ĒŖ╣ļ░£ņä▒ ņåīĒÖöņä▒ ĻČżņ¢æ)ņŚÉņä£ļŖö ņןĻĖ░Ļ░ä PPIļź╝ ņé¼ņÜ®ĒĢśļŖö Ļ▓āņØ┤ ņÜöĻĄ¼ļÉ£ļŗż[9]. ņĢ×ņä£ ĻĖ░ņ×¼ĒĢ£ ļŗżļźĖ ņĢĮņĀ£ņÖĆ ļ│æņÜ®ĒĢśļŖö ļÅÖņĢł, PPIļŖö ĒĢ┤ļŗ╣ ņøÉņØĖ ņĢĮļ¼╝ņØ┤ ĒĢäņÜöĒĢ£ ĻĖ░Ļ░äļÅÖņĢł ņ▓śļ░®ļÉśņ¢┤ņĢ╝ ĒĢ£ļŗż.
ņ×¼ņČ£Ēśł Ļ┤Ćļ”¼(management of recurrent bleeding)
ņČ£Ēśł Ēøä ņä▒Ļ│ĄņĀüņØĖ ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņ×¼ņČ£ĒśłņØ┤ ļ░£ņāØĒĢĀ Ļ▓ĮņÜ░ ļ░śļ│Ą ļé┤ņŗ£Ļ▓Į ņŗ£Ē¢ē ļ░Å ņ¦ĆĒśłņłĀņØ┤ ĻČīĻ│ĀļÉ£ļŗż[11,12]. ļ░śļ│Ą ļé┤ņŗ£Ļ▓Į ļ░Å ņ¦ĆĒśłņłĀņØĆ ņłśņłĀņŚÉ ļ╣äĒĢ┤ ņ×¼ņČ£ĒśłļźĀņØĆ ļåÆņĢśņ£╝ļéś ņé¼ļ¦ØļźĀņŚÉļŖö ņ£ĀņØśĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłĻ│Ā, ĒĢ®ļ│æņ”ØņØĆ ļŹö ņĀüņØĆ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[49]. ņ×¼ņČ£Ēśł ņŗ£ ļ░śļ│Ą ļé┤ņŗ£Ļ▓ĮņØ┤ ļČłĻ░ĆļŖźĒĢĀ Ļ▓ĮņÜ░ļéś ļé┤ņŗ£Ļ▓Į ņ¦ĆĒśłņłĀņŚÉ ņŗżĒī©Ē¢łņØä Ļ▓ĮņÜ░ņŚÉļŖö Ļ▓ĮļÅÖļ¦ź ņāēņĀäņłĀ(transcatheter arterial embolization, TAE)ņØä ņÜ░ņäĀņĀüņ£╝ļĪ£ Ļ│ĀļĀżĒĢĀ ņłś ņ׳ļŗż[10-12]. ņĄ£ĻĘ╝ ņŖżņø©ļŹ┤ņŚÉņä£ ļ░£Ēæ£ĒĢ£ ņĮöĒśĖĒŖĖ ļČäņäØņŚÉ ļö░ļź┤ļ®┤, TAEļŖö ņłśņłĀņŚÉ ļ╣äĒĢ┤ ņé¼ļ¦ØļźĀņŚÉņä£ ņ£ĀņØśĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņ£╝ļ®┤ņä£ ņČöĻ░Ć ņČ£Ēśł, ĒĢ®ļ│æņ”Ø ļ░£ņāØ, ņ×ģņøÉ ĻĖ░Ļ░äņŚÉņä£ ļŹö ņÜ░ņłśĒĢ£ Ļ▓░Ļ│╝ļź╝ ļ│┤ņśĆļŗż[50].
Ļ▓░ ļĪĀ
NVUGIBļŖö ļé┤ņŗ£Ļ▓ĮņØä ņŗ£Ē¢ēĒĢśļŖö ņØśņé¼Ļ░Ć ĒØöĒ׳ ņĀæĒĢśļŖö ņØæĻĖē ņāüĒÖ® ņżæ ĒĢśļéśļĪ£ ļé┤ņŗ£Ļ▓Į ĻĖ░ĻĖ░ņÖĆ ņĢĮņĀ£ņØś ļ░£ļŗ¼ņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņŚ¼ņĀäĒ׳ ļåÆņØĆ ņØ┤ĒÖśņ£© ļ░Å ņé¼ļ¦ØļźĀņØä ļ│┤ņØ┤ļŖö ņ¦łĒÖśņØ┤ļŗż. NVUGIB ĒÖśņ×ÉĻ░Ć ļé┤ņøÉĒ¢łņØä ļĢī, ņ╣śļŻīļŖö ļé┤ņŗ£Ļ▓Į ņĀä, ņŗ£ņłĀ ņżæ, ļ░Å ņŗ£ņłĀ ĒøäņØś ņäĖ ņŗ£ņĀÉņ£╝ļĪ£ ļéśļłäņ¢┤ņä£ ņ¦äĒ¢ēļÉ£ļŗż. ņĄ£ĻĘ╝ ņśüĻĄŁņØś ļ│┤Ļ│ĀņŚÉ ļö░ļź┤ļ®┤ NVUGIBļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉņØś 30ņØ╝ ņé¼ļ¦ØļźĀņØĆ 7.0%ņŚÉ ļŗ¼ĒĢśļ®░, ņé¼ņØĖņØĆ ņČ£Ēśł ņ×Éņ▓┤ļ│┤ļŗżļŖö ļÅÖļ░śļÉ£ ņŗ¼ĒśłĻ┤Ć ņ¦łĒÖśņŚÉ ĻĖ░ņØĖĒĢ£ Ļ▓āņ£╝ļĪ£ ļéśĒāĆļé¼ļŗż[51]. ņØ┤ļŖö NVUGIB ĒÖśņ×É ņ╣śļŻī ņŗ£ ņČ£Ēśł Ļ┤Ćļ”¼ļ┐Éļ¦ī ņĢäļŗłļØ╝ ļÅÖļ░śļÉ£ ĒĢ®ļ│æņ”Ø Ļ┤Ćļ”¼ņØś ņżæņÜöņĀÉņØä ņŗ£ņé¼ĒĢ£ļŗż. ļö░ļØ╝ņä£ NVUGIBņØś ļŗżņ¢æĒĢ£ ņøÉņØĖĻ│╝ ļ│æĒā£ņāØļ”¼ļź╝ Ļ│ĀļĀżĒĢśņŚ¼ Ļ░ü ĒÖśņ×ÉņŚÉ ļ¦×ļŖö Ļ░£ļ│äņĀüņØĖ ņ£äĒŚśļÅä ĒÅēĻ░ĆņÖĆ ņāüĒā£ņŚÉ ļö░ļźĖ ņĀüņĀłĒĢ£ ņ╣śļŻī ņĀæĻĘ╝ļ▓ĢņØä ņ░ŠļŖö Ļ▓āņØ┤ ņżæņÜöĒĢśļ®░, Ļ░£ņØĖ ļ¦×ņČżĒśĢ ļé┤ņŗ£Ļ▓Į ņ╣śļŻī ļ░Å ņØ┤Ēøä Ļ┤Ćļ”¼ ņĀäļץņØś ņłśļ”ĮņØ┤ ĒĢäņłśņĀüņØ┤ļØ╝ ĒĢśĻ▓Āļŗż.