Gastric cancer is the fifth most common cancer and the third leading cause of cancer-related mortality globally. [1] Although the age-standardized incidence rates of gastric cancer in Korea are high, the ratio of gastric cancer-related mortality to incidence is much lower in Korea than in other countries. [2] It is attributable to the emphasis on early detection and treatment of gastric cancer through the National Cancer Screening Program (NCSP) for gastric cancer, which was launched in Korea in 2002. [3] The NCSP for gastric cancer invites all Koreans aged Ōēź40 years to undergo endoscopy or upper gastrointestinal series every 2 years. Helicobacter pylori (H. pylori) is recognized as a definite carcinogen, based on the criteria established by the International Agency for Research on Cancer, the specialized cancer agency of the World Health Organization. It is acknowledged as the single most important etiopathogenetic contributor to gastric adenocarcinoma. [4] A recent systematic review and meta-analysis of 10 randomized controlled trials performed in either Asia or South America reported that H. pylori eradication reduced the incidence of gastric cancer by 46.0%, with the number needed to treat of 72 to prevent one case and reduced mortality of gastric cancer by 39.0%. [5] Therefore, in addition to early detection of gastric cancer through NCSP, screening for H. pylori infection and eradication therapy can further reduce the incidence and mortality of gastric cancer.
The Kyoto classification of gastritis was introduced in 2013 as an endoscopic classification of gastritis established by the Japan Gastroenterological Endoscopy Society. [6] The Kyoto classification scores are used to determine H. pylori infection and predict the risk of gastric cancer based on evaluation of the gastric mucosa. [7] The classification system includes 23 endoscopic features associated with gastritis, including atrophy, intestinal metaplasia, and regular arrangement of collecting venules (RAC). [6] Of these, atrophy, intestinal metaplasia, enlarged folds, and nodularity are correlated with gastric cancer risk. Furthermore, diffuse redness with or without RAC, is associated with H. pylori infection. [6] The Kyoto classification score for gastritis is the sum of scores for the five aforementioned endoscopic parameters and ranges from 0 to 8.
Several studies have confirmed the usefulness of Kyoto classification scores for diagnosis of H. pylori infection and estimation of the gastric cancer risk. The Kyoto classification scores showed an excellent area under the receiver operating characteristic (ROC) curve (0.886) for prediction of H. pylori infection with a cut-off value of 2 in participants with a negative or high H. pylori antibody titer. [8] A Kyoto classification score of Ōēź2 could predict H. pylori infection with an accuracy of 90.0%. [8] H. pylori infection rates in individuals with Kyoto classification scores of 0, 1, and Ōēź2 were 1.5%, 45.0%, and 82.0%, respectively among 870 participants without a history of H. pylori eradication therapy. [9] Specifically, diffuse redness of the gastric mucosa showed a good positive predictive value (65.6~91.5%) for H. pylori infection, and RAC showed high sensitivity for non-infection (86.7~100.0%). [10-12] This classification system is useful to predict the risk of gastric cancer and H. pylori infection. Among the Kyoto classification variables, gastric atrophy (open-type) was associated with gastric cancer (OR, 7.2~14.2). [13,14]
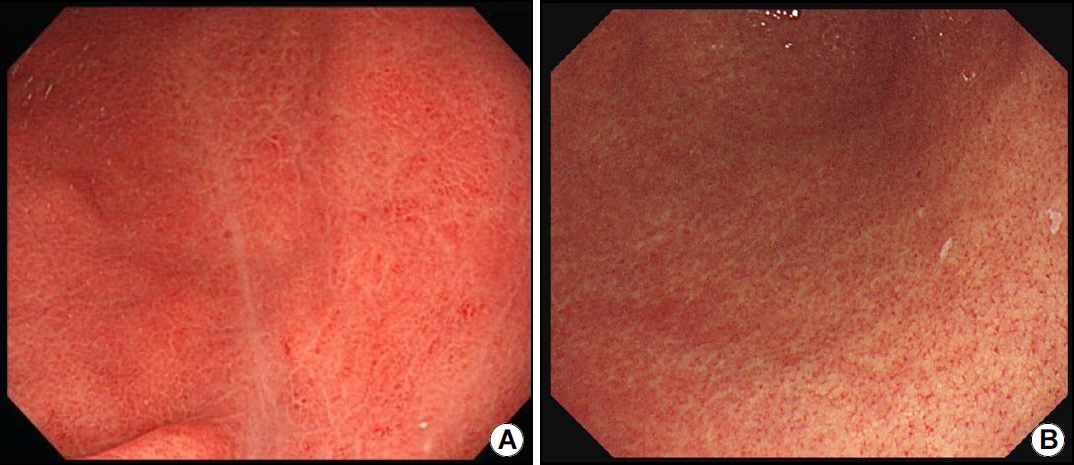
This issue includes a study by Kang et al., [15] which investigated the usefulness of the Kyoto classification score for prediction of H. pylori infection based on endoscopic features. The authors investigated 317 H. pylori-positive and 370 H. pylori-negative individuals. They retrospectively analyzed endoscopic images and recorded scores based on the Kyoto classification of gastritis. The ideal cut-off value of the Kyoto classification score based on the ROC curve analysis was 2 points, which was similar to the cut-off values reported by previous studies. A Kyoto classification score of Ōēź2 showed a sensitivity of 95.27%, a sensitivity of 63.78%, positive predictive value of 69.27%, and negative predictive value of 94.02% for diagnosis of H. pylori infection. Nodularity (OR, 24.69; 95% CI, 8.57~71.16) and severe diffuse redness (OR, 30.82; 95% CI, 14.07~67.52) showed the highest OR for detecting H. pylori infection on multivariate analysis. Nodularity leads to a goose skin-like appearance in the antrum, and histopathological evaluation of biopsy specimens shows lymphoid follicles or significant inflammatory cell infiltration. This condition is more commonly observed in young women, and an association with diffuse gastric cancer has been reported. [16] Diffuse redness is primarily observed in the non-atrophic mucosa of the gastric corpus. It is uniform in distribution with microscopic redness in the fundic glands (Fig. 1). Spotty redness, another characteristic of H. pylori infection, appears mainly as distinct bleeding spots distributed across the fundus (Fig. 2). As observed in the figures, these findings improve after eradication therapy. Notably, acid-suppression therapy is associated with high false-negative rates on H. pylori testing; therefore, endoscopy may be a useful complementary diagnostic tool. [17]
This is a meaningful study, which highlights the usefulness of the Kyoto classification score for detecting H. pylori infection in Korea. An early diagnosis of clinical suspicion and consequently, early diagnosis of H. pylori infection based on endoscopic findings is particularly important in Korea because all adults aged >40 undergo endoscopy every 2 years per the NCSP recommendations. Confirmatory tests and eradication therapy in patients with endoscopically suspected H. pylori infection can significantly reduce the incidence and mortality of gastric cancer in the future. It might be a cost-effective method for gastric cancer prevention. The aforementioned endoscopic findings will be widely used for diagnosing H. pylori infection using artificial intelligence and image-enhanced endoscopic techniques including as magnifying narrowband imaging and linked color imaging endoscopy. [18]