서 론
상부위장관 출혈은 종종 치명적일 수 있으며, 응급실로 내원하는 중요한 원인 중 하나이다[1]. 상부위장관 출혈의 가장 흔한 원인으로는 위궤양과 십이지장 궤양이 있으며, 이외에도 식도 혹은 위정맥류, Mallory-Weiss tear, Dieulafoy’s lesion 등이 있다[2]. 그 외 상부위장관 출혈의 드문 원인으로 내장 가성동맥류 출혈이 있다.
내장 가성동맥류는 복부 수술과 췌장염, 외상 등의 합병증으로 인해 발생하는 것으로 알려져 있다[3,[4]]. 내장 가성동맥류에 의한 위장관 출혈은 드물지만, 내장 가성동맥류의 파열이나 출혈이 발생할 경우 이에 의한 사망률은 25%에서 70%로 보고되고 있다[5,6]. 내장 가성동맥류 중의 대다수는 60%를 차지하는 비장 가성동맥류이며, 좌위 가성동맥류는 4% 미만으로 그 빈도가 낮다[7]. 내장 가성동맥류의 파열이나 출혈은 주로 복강내 출혈이나 hemosuccus pancreaticus, 위장관 출혈로 나타날 수 있다. 그 중 좌위 가성동맥류에 의한 위장관 출혈은 드물며, 특히 위궤양 출혈로 나타나는 경우는 매우 드물게 보고되고 있다[8,9]. 본고에서는 복부 수술이나 췌장염, 외상의 과거력이 없는 환자에서 발생한, 좌위 가성동맥류와 관련된 위궤양 출혈 1예를 보고하고자 한다.
증 례
77세 남자가 하루 전부터 발생한 어지럼증과 24시간 동안 세 차례 발생한 흑색변으로 응급실을 통해 입원하였다. 기저질환으로 고혈압과 당뇨병, 협심증이 있었고, 한 달 전 불안정형 협심증에 대하여 경피적 관상동맥 중재술을 시행받은 후 이중 항혈소판제 요법을 시작하였다. 9개월 전 건강검진 목적으로 시행한 상부위장관 내시경에서 위축성 위염 외 특이 소견은 없었다.
내원 당시 활력징후는 혈압 90/55 mmHg, 맥박 109회/분, 호흡수 20회/분이었다. 복부 진찰에서 복부는 부드러웠고 압통이나 반발통은 없었다.
말초혈액 검사에서 혈색소 8.7 g/dL, 혈소판 283,000/mm3였고, 혈액응고인자 검사에서 prothrombin time-international normalized ratio 1.24였다. 혈청 생화학 검사에서 BUN 45 mg/dL, amylase 36 U/L, lipase 58 U/L, AST/ALT 14/14 IU/L, 크레아티닌 1.33 mg/dL였다. 혈청 헬리코박터 파일로리 항체 IgG는 음성이었다.
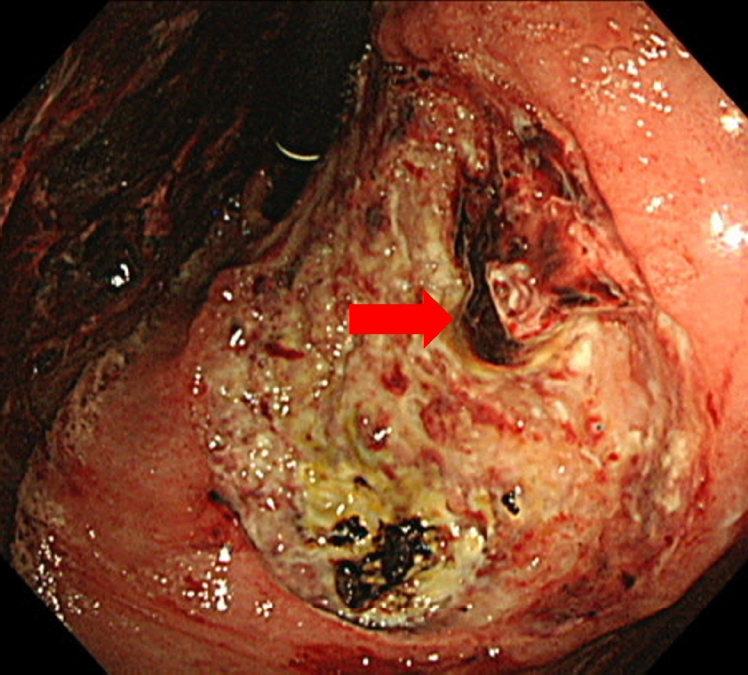
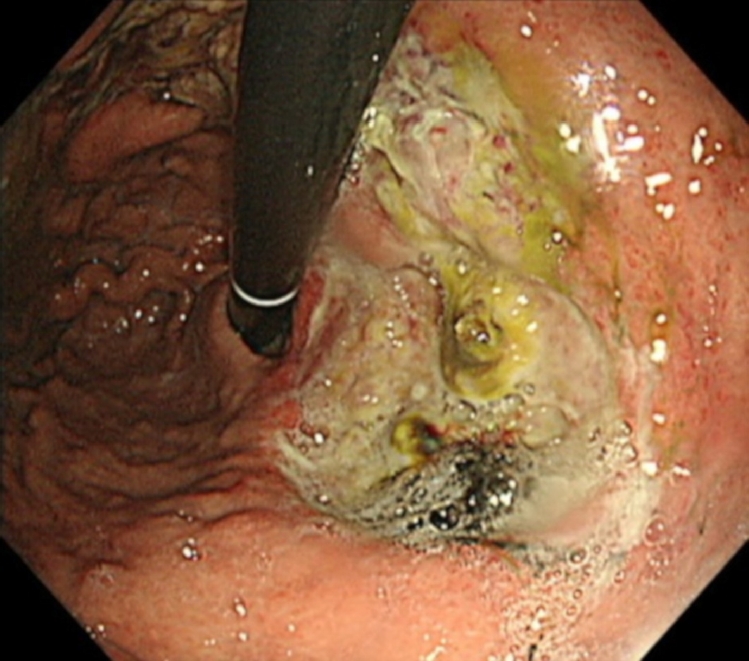
응급 상부위장관 내시경시 위 상체부의 소만에 3 cm 크기의 궤양이 있었고, 궤양 안에 출혈이 동반된 박동성 상피하종양 모양의 병변이 관찰되었다(Fig. 1). 지혈술로 내시경적 에피네프린 국소 주사법과 내시경적 fibrin glue 국소 주사법, 전기응고술이 시행되었고, 시술 후 지혈되어 내시경을 종료하고 경과를 보기로 하였다. 내시경 시술 3일 후, 환자는 다량의 토혈로 인한 저혈량 쇼크가 발생하였다. 응급 혈관조영술을 시행하였고, 상장간동맥조영술에서 좌위동맥에서 조영제의 누출 소견을 보이는 주머니모양동맥류가 관찰되었다(Fig. 2). 가성동맥류에 의한 위 출혈로 진단하고 좌위동맥을 코일을 이용하여 색전술을 시행하였고, 시술 후 혈관조영술에서 출혈 소견은 관찰되지 않았다. 이후 환자는 더 이상의 위장관 출혈을 보이지 않았다. 3일 후 시행한 상부위장관 내시경에서 삼출물로 덮여 있는 궤양이 관찰되었고 좌위 가성동맥류였던 상피하종양 모양의 병변은 더 이상 보이지 않았다(Fig. 3). 두 달 후 환자는 추적 관찰 상부위장관 내시경을 받았고 위궤양은 치유기로 확인되었고 추가적인 출혈 없이 안정적으로 외래를 통한 추적 관찰 중이다.
고 찰
내장 가성동맥류는 외상이나 의인성 손상, 국소 염증, 감염 등에 의해 발생한다고 알려져 있으며[10], 특히 복부 수술이나 외상, 췌장염의 합병증으로 주로 발생한다[3,4]. 내장 가성동맥류의 가장 흔한 원인은 만성 췌장염으로 알려져 있는데, 특히 비장 가성동맥류와 관련이 깊다[11]. 내장 가성동맥류와 연관된 위장관 출혈은 드물지만 환자에게 치명적일 수 있다. 내장 가성동맥류 중 비장 가성동맥류에 의한 위장관 출혈은 증례들이 출판되어 있고, 한 증례 모음(case series)에서 비장 가성동맥류 환자 10명 중 2명이 위 출혈을 보였다고 보고된 바 있다[12]. 그러나 좌위 가성동맥류에 의한 위장관 출혈은 매우 드물어, 증례 모음이나 임상 연구가 보고된 바 없다. 이는 비장 가성동맥류가 전체 내장 가성동맥류 중 60%로 가장 많이 차지하고 있는 반면, 좌위 가성동맥류는 4% 미만으로 그 빈도가 낮기 때문으로 보인다[7]. 특히 좌위 가성동맥류와 관련된 위궤양 출혈은 더욱 드물어, 증례 보고가 두 건에 불과하다[8,9].
좌위 가성동맥류와 연관된 위궤양 출혈은 Clemens [8]에 의해 처음 보고되었다. 하지만 당시 소화기 내시경이 널리 통용되지 않았기 때문에 내시경 영상은 기록되지 않았다. 수술을 통해 얻어진 조직의 병리 소견에서 위궤양과 미란과 함께 파열된 가성 동맥류(eroded and rupture pseudoaneurysm)가 확인되었다. Sudo 등[9]은 좌위 가성동맥류와 관련된 위궤양 내시경 영상을 보고하였는데 본 증례에서와 마찬가지로 큰 위궤양이 상체부의 소만에 위치하였고, 궤양 내부에 상피하종양 모양의 병변이 관찰되었다. 혈관색전술 후 가성동맥류로 판단하였던 상피하종양 모양의 병변은 소실되었다.
본 증례 환자는 가성동맥류의 흔한 원인으로 알려져 있는 복부 수술력이나 외상, 췌장염의 과거력이 없었고, 한 달 전 불안정형 협심증에 대하여 경피적 관상동맥 중재술 후 이중 항혈소판제 요법(아스피린 100 mg 하루 1회와 클로피도그렐 75 mg 하루 1회 병합요법)을 시작하였다. 아스피린은 프로스타글란딘을 억제하거나 위장관 점막에 직접 손상시킴으로써 위, 십이지장 궤양을 유발할 수 있다[13]. 클로피도그렐이 위, 십이지장 궤양을 유발하는지에 대해서는 다소 불명확하다. 그러나 이중 항혈소판제 요법이 아스피린 단독 투여보다 위장관 출혈을 발생시킨다고 알려져 있다[14,15]. 또한, 이중 항혈소판제 요법이 아스피린 단독 투여보다 위, 십이지장 궤양을 더 유발한다는 연구도 보고된 바 있다[16]. 이는 클로피도그렐이 위, 십이지장 궤양을 직접적으로 유발하지는 않지만, 혈소판 표면의 ADP를 통해 adenosine cyclase를 억제시켜 아스피린이 손상시킨 위, 십이지장 점막의 치유를 지연시키기 때문으로 보인다.
본 증례 환자의 경우에도 한 달 전 시작한 이중 항혈소판제 요법이 위궤양 발생에 주요한 역할을 했던 것으로 판단된다. 진행된 위궤양이 비장동맥에 미란을 일으켜 가성동맥류를 유발하는 경우로 보이는 증례들이 보고된 바 있다[17,18]. 위궤양이 좌위 가성동맥류를 유발한 증례는 아직 보고된 바 없지만, 본 증례 환자의 경우 한 달간 투여된 이중 항혈소판제 요법에 의해 유발된 진행된 위궤양이 좌위동맥에 미란을 일으켜 가성동맥류가 형성된 것으로 추정된다.
내장 가성동맥류에 의한 출혈은 혈관색전술이 우선 권장되고, 만일 혈관색전술로 지혈이 안된다면 수술적 치료가 필요하다[6,10]. 가성동맥류에 의한 출혈은 환자에게 치명적일 수 있으므로, 좌위 가성동맥류와 연관된 위궤양 출혈이 발생할 경우 이를 일찍 의심하고 그에 알맞은 치료를 하는 것이 중요하겠다[9].
요약하자면 위궤양 출혈 환자에서 복부 수술력이나 외상, 췌장염 등 가성동맥류를 유발할 만한 원인이 없더라도 크기가 큰 궤양이 위 상체부에 위치하여 있고, 그 내부에 박동성 상피하종양 모양의 병변이 있다면 좌위 가성동맥류를 고려해보는 것이 필요하겠다.