ņä£ ļĪĀ
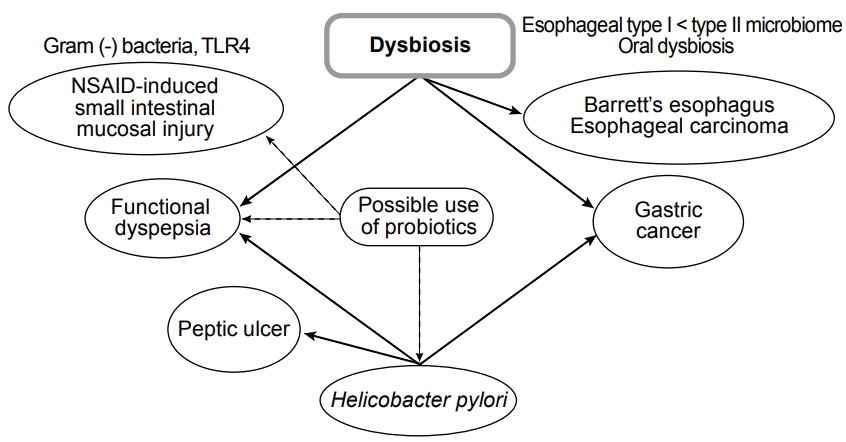
ņןļé┤ ņäĖĻĘĀņ┤ØņØĆ ņØĖĻ░äņØś ļīĆņé¼ ĻĖ░ļŖźĻ│╝ ļ®┤ņŚŁ ĻĖ░ļŖźņŚÉ ņżæņÜöĒĢ£ ņŚŁĒĢĀņØä ĒĢśļ®░, ņןļé┤ ņäĖĻĘĀņ┤ØņØś ņØ┤ņāüņØĆ ņŚ╝ņ”Øņä▒ ņןņ¦łĒÖśņØ┤ļéś Ļ│╝ļ»╝ņä▒ ņןņ”ØĒøäĻĄ░Ļ│╝ Ļ░ÖņØĆ ņåīĒÖöĻĖ░ ņ¦łĒÖś ņØ┤ņÖĖņŚÉļÅä ļ╣äļ¦ī, ļŗ╣ļć©, ņŚ╝ņ”Ø ļ░Å ļīĆņé¼ņä▒ ņ¦łĒÖś, ņ×ÉĻ░Ćļ®┤ņŚŁ ņ¦łĒÖś, Ē¢ēļÅÖ ņØ┤ņāü, ļÅÖļ¦źĻ▓ĮĒÖöņ”Ø ļō▒ņØś ļŗżņ¢æĒĢ£ ņ¦łĒÖśļōżĻ│╝ ņŚ░Ļ┤ĆļÉ£ļŗż[1]. ņāüļČĆņ£äņןĻ┤Ć ņ¦łĒÖś ņżæņŚÉņä£ļŖö Helicobacter pylori (H. pylori) Ļ░ÉņŚ╝ņØ┤ ņ£äņŚ╝ ļ░Å ņ£äņĢö ļ░£ņāØņŚÉ Ļ┤ĆņŚ¼ĒĢśļŖö ĻĖ░ņĀäņØ┤ ņל ņĢīļĀżņĀĖ ņ׳ņ£╝ļ®░ ņ£ä ņäĖĻĘĀņ┤ØņØś ņØ┤ņāüņØ┤ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØĻ│╝ ņŚ░Ļ┤ĆļÉ£ļŗżļŖö ņŚ░ĻĄ¼ļÅä ņ׳ļŗż[2,3]. ļśÉĒĢ£ ļ░öļĀøņŗØļÅäņÖĆ ļ╣äņŖżĒģīļĪ£ņØ┤ļō£ņåīņŚ╝ņĀ£(nonsteroidal anti-inflammatory drug, NSAID)ņŚÉ ņØśĒĢ£ ņåīņן ņĀÉļ¦ē ņåÉņāü ļ░£ņāØ ĻĖ░ņĀäņŚÉļÅä ņןļé┤ ņäĖĻĘĀņ┤ØņØ┤ Ļ┤ĆņŚ¼ĒĢ£ļŗż(Fig. 1) [4,5]. ņØ┤ļ¤¼ĒĢ£ ņןļé┤ ņäĖĻĘĀņ┤Ø ņØ┤ņāüĻ│╝ ņŚ░Ļ┤ĆļÉśļŖö ņ¦łĒÖśņØś ņ╣śļŻī ļ░®ļ▓Ģ ņżæ ĒĢśļéśļĪ£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖż(probiotics)Ļ░Ć ņé¼ņÜ®ļÉĀ ņłś ņ׳ļŗż. ļ│ĖĻ│ĀņŚÉņä£ļŖö ņāüļČĆņ£äņןĻ┤Ć ņ¦łĒÖśņŚÉņä£ ņןļé┤ ņäĖĻĘĀņ┤ØņØś ņŚŁĒĢĀĻ│╝ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņØś ņĀüņÜ®ņŚÉ ļīĆĒĢśņŚ¼ ņé┤ĒÄ┤ļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ļ│Ė ļĪĀ
1. ņןļé┤ ņäĖĻĘĀņ┤Ø
ņØĖĻ░äņØś ĻĄ¼Ļ░ĢļČĆĒä░ ļīĆņןĻ╣īņ¦Ć ļ¬©ļōĀ ņåīĒÖöĻ┤ĆņŚÉ ņäĖĻĘĀņØ┤ ņĪ┤ņ×¼ĒĢśņ¦Ćļ¦ī ĻĘĖ ļīĆļČĆļČäņØĆ ļīĆņןņŚÉ ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ņןļé┤ ņäĖĻĘĀņ┤Ø ņŚ░ĻĄ¼ļŖö ņŻ╝ļĪ£ ļīĆļ│ĆņØä ņØ┤ņÜ®ĒĢśņŚ¼ ņ¦äĒ¢ēļÉśĻ│Ā ņ׳ļŗż. ņØĖĻ░äņØś ņןļé┤ ņäĖĻĘĀņØĆ ņ▓┤ņäĖĒżņłśļ│┤ļŗż ņĢĮ 10ļ░░ ļ¦ÄņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ņ£╝ļéś, ņØ┤ ņł½ņ×ÉļŖö ņśżļלļÉ£ ļģ╝ļ¼ĖņØś ļīĆļץņĀüņØĖ Ļ│äņé░ Ļ▓░Ļ│╝ņŚÉ ĻĘ╝Ļ▒░ĒĢśĻ│Ā ņ׳ļŗż[6]. ņĄ£ĻĘ╝ ņāłļĪ£ņÜ┤ Ļ│äņé░ ļ░®ļ▓ĢņØä ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņ▓┤ņäĖĒżņłśņÖĆ ņןļé┤ ņäĖĻĘĀņłśĻ░Ć 1:1ņŚÉ ĻĘ╝ņĀæĒĢśņŚ¼ ļé©ņ×ÉņØś Ļ▓ĮņÜ░ 1.3:1 (38├Ś1012:30├Ś1012), ņŚ¼ņ×ÉņØś Ļ▓ĮņÜ░ 2.2:1 (44├Ś1012:21├Ś1012)ļĪ£ Ļ│äņé░ļÉśņŚłļŗż[7]. ņĄ£ņŗĀ ĻĖ░ļ▓ĢņØĖ 16S rRNA ņ░©ņäĖļīĆ ņŚ╝ĻĖ░ ļČäņäØ(next generation sequencing) ļ░®ļ▓Ģņ£╝ļĪ£ Ļ▓ĆņČ£ļÉ£ ņןļé┤ ņäĖĻĘĀņØś ņĢĮ 80%ļŖö ļ░░ņ¢æņØ┤ ļČłĻ░ĆļŖźĒĢśĻ▒░ļéś ņĢäņ¦üĻ╣īņ¦Ć ļ░░ņ¢æņØ┤ ļÉśņ¦Ć ņĢŖņØĆ ĻĘĀņØ┤ļŗż[8]. ņØĖĻ░äņØś ļŗ©ļ░▒ņ¦ł ņĮöļö® ņ£ĀņĀäņ×ÉļŖö ņĢĮ 20,000Ļ░£ņŚÉ ļČłĻ│╝ĒĢśņ¦Ćļ¦ī ņןļé┤ ņäĖĻĘĀņ┤ØņØś ļŗ©ļ░▒ ņĮöļö® ņ£ĀņĀäņ×ÉļŖö ņĢĮ 100,000Ļ░£ļĪ£ ņØĖĻ░äņØś ļīĆņé¼ ĻĖ░ļŖź ņżæ ļ¦ÄņØĆ ļČĆļČäņØä ņןļé┤ ņäĖĻĘĀņ┤ØņØ┤ ļŗ┤ļŗ╣ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[9]. ļ¼┤ĻĘĀ ņāüĒā£ņØś Ēā£ņĢäĻ░Ć ņé░ļ¬©ņØś ņé░ļÅäļź╝ ĒåĄĒĢśņŚ¼ ņČ£ņāØĒĢśļŖö Ļ│╝ņĀĢņŚÉņä£ ņןļé┤ ņäĖĻĘĀņØś ņĀĢņ░®ņØ┤ ņŗ£ņ×æļÉśļŖöļŹ░, ņĀ£ņÖĢņĀłĻ░£ļź╝ ĒåĄĒĢśņŚ¼ Ēā£ņ¢┤ļéśļŖö ņŗĀņāØņĢäņÖĆ ņ¦łņŗØ ļČäļ¦īņ£╝ļĪ£ Ēā£ņ¢┤ļé£ ņŗĀņāØņĢäļŖö ņןļé┤ ņäĖĻĘĀļōżņØ┤ ņĀĢņ░®ļÉśļŖö ņł£ņä£Ļ░Ć ļŗżļź┤ļŗż. ņןļé┤ ņäĖĻĘĀņ┤ØņØĆ ņĢĮ 3ņäĖĻ▓ĮņŚÉ ņä▒ņØĖĻ│╝ ņ£Āņé¼ĒĢ£ ņłśņżĆņ£╝ļĪ£ ļ░£ļŗ¼ĒĢśĻ▓ī ļÉśņ¢┤ ņä▒ņØĖĻĖ░ņŚÉļŖö ņØ╝ņĀĢĒĢśĻ▓ī ņ£Āņ¦ĆļÉśĻ│Ā, ņ£äņןĻ┤Ć ņāØļ”¼ĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ļéśĒāĆļéśļŖö 70ņäĖ ņØ┤ņāüņØś Ļ│ĀļĀ╣ņØ┤ ļÉśļ®┤ņä£ ņןļé┤ ņäĖĻĘĀņ┤ØņØś ņĪ░ņä▒ļÅä ļ│ĆĒÖöļÉśĻĖ░ ņŗ£ņ×æĒĢ£ļŗż. ņןļé┤ ņäĖĻĘĀņ┤ØņØś ņĪ░ņä▒ņØĆ ņØīņŗØ, ĒÖśĻ▓Į, ĒĢŁņāØņĀ£, ņĢĮņĀ£ ļō▒ ņŚ¼ļ¤¼ ņÜöņØĖņŚÉ ņśüĒ¢źņØä ļ░øņĢä ņØ╝ņŗ£ņĀüņ£╝ļĪ£ ļ│ĆĒĢĀ ņłś ņ׳ļŖöļŹ░[10], ļ¦īņĢĮ ņØ┤ļ¤░ ļ│ĆĒÖöĻ░Ć ĒÜīļ│ĄļÉśĻĖ░ ņ¢┤ļĀżņÜĖ ņĀĢļÅäļĪ£ ļäłļ¼┤ ņŗ¼ĒĢśĻ▒░ļéś ņśżļל ņ¦ĆņåŹļÉśļ®┤ ņןļé┤ ņäĖĻĘĀņ┤ØņØś ĻĘĀĒśĢņØ┤ Ļ╣©ņ¦ĆĻ▓ī ļÉśņ¢┤ ņןļé┤ ņäĖĻĘĀ ļČłĻĘĀĒśĢ(dysbiosis)ņØ┤ ļ░£ņāØĒĢśĻ▓ī ļÉ£ļŗż[11].
2. ņŗØļÅä ņäĖĻĘĀņ┤ØĻ│╝ ņŗØļÅäņĢö
ņŗØļÅäļŖö ņŗØļÅä ņāüņ×¼ĻĘĀ, ĻĄ¼Ļ░ĢņŚÉņä£ ļäśņ¢┤ņś© ĻĘĀ ļśÉļŖö ņ£äņŚÉņä£ ņŚŁļźśļÉ£ ĻĘĀņŚÉ ļģĖņČ£ļÉ£ļŗż. ņŚŁļźśņä▒ ņŗØļÅäņŚ╝Ļ│╝ ļ░öļĀøņŗØļÅäņÖĆ Ļ░ÖņØ┤ ļ¦īņä▒ņĀüņØĖ ņŚ╝ņ”ØņŚÉ ņØśĒĢśņŚ¼ ņŗØļÅä ņĀÉļ¦ē ņåÉņāüņØ┤ ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░ ņĀÉļ¦ēĒĢś ņĪ░ņ¦üņØ┤ ņŗØļÅä ņäĖĻĘĀņ┤ØņŚÉ ņśüĒ¢źņØä ļ░øņØä ņłś ņ׳ļŗż[4]. ņŗØļÅä ņäĖĻĘĀņ┤ØņØĆ ļæÉ ĻĄ░ņ£╝ļĪ£ ļéśļłäņ¢┤ņ¦ł ņłś ņ׳ļŖöļŹ░ IĒśĢ ņäĖĻĘĀņ┤ØņØĆ ņŻ╝ļĪ£ StreptococcusļĪ£ ĻĄ¼ņä▒ļÉśļ®░ ņĀĢņāü ņŗØļÅäņŚÉņä£ Ļ┤Ćņ░░ļÉ£ļŗż. IIĒśĢ ņäĖĻĘĀņ┤ØņØĆ Veillonella, Prevotella, Haemophilus, Neisseria, Rothia, Granulicatella, Campylobacter, Porphyromonas, Fusobacterium, ActinomycesņÖĆ Ļ░ÖņØĆ ĻĘĖļ×ī ņØīņä▒ ĒśÉĻĖ░ņä▒ Ēś╣ņØĆ ļ»ĖĒśĖĻĖ░ņä▒(microaerophiles) ĻĘĀļōżļĪ£ ņŗØļÅäņŚ╝(odds ratio [OR], 15.4)ņØ┤ļéś ļ░öļĀøņŗØļÅä(OR, 16.5)ņÖĆ Ļ░ÖņØĆ ļ╣äņĀĢņāü ņŗØļÅäņÖĆ ņŚ░Ļ┤ĆļÉ£ļŗż[12]. ĒĢśļČĆ ņŗØļÅä ņäĖĻĘĀņ┤ØņØ┤ IĒśĢņŚÉņä£ IIĒśĢņ£╝ļĪ£ ņ¦äĒ¢ēĒĢśļŖö Ļ▓āņØĆ NF-kB Ļ▓ĮļĪ£ļź╝ ĒåĄĒĢśņŚ¼ ņŚ╝ņ”Ø ļ░śņØæņØ┤ ņ£Āļ░£ļÉśļ®┤ņä£ ņŗØļÅäņŚ╝ņŚÉņä£ ļ░öļĀøņŗØļÅäļź╝ Ļ▒░ņ│É ņŗØļÅäņäĀņĢöņØ┤ ļ░£ņāØĒĢśļŖö ņ¦äĒ¢ē Ļ│╝ņĀĢņŚÉ ņŚ░Ļ┤ĆļÉśļŖö Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż[4]. ĻĄ¼Ļ░Ģ ņäĖĻĘĀņ┤ØĻ│╝ ņŗØļÅäņĢöņØś Ļ┤ĆĻ│äļź╝ ņĪ░ņé¼ĒĢ£ ņżæĻĄŁ ņŚ░ĻĄ¼ņŚÉņä£ ĻĄ¼Ļ░Ģ ļé┤ Tannerella forsythiaņØś ņ”ØĻ░ĆĻ░Ć ņŗØļÅäņäĀņĢö ņ£äĒŚśņä▒Ļ│╝ ņŚ░Ļ┤ĆļÉśņŚłĻ│Ā Porphyromonas gingivalis ņØś ņ”ØĻ░ĆļŖö ņŗØļÅäĒÄĖĒÅēņāüĒö╝ņäĖĒżņĢö ņ£äĒŚśņä▒Ļ│╝ ņŚ░Ļ┤ĆļÉśņŚłļŗż[13]. ņżæĻĄŁņØś ļŗżļźĖ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĻĄ¼Ļ░Ģ ļé┤ Lautropia, Bulleidia, Catonella, Corynebacterium, Moryella, Peptococcus ļ░Å CardiobacteriumņØś Ļ░ÉņåīĻ░Ć ņŗØļÅäĒÄĖĒÅēņāüĒö╝ņäĖĒżņĢö ļ░£ņāØĻ│╝ ņŚ░Ļ┤ĆļÉśņŚłļŗż[14]. ņØ┤ļ×Ć ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņŗØļÅäņŚ╝ ĒÖśņ×Éļéś Ļ▒┤Ļ░ĢņØĖņŚÉ ļ╣äĒĢśņŚ¼ ņŗØļÅäĒÄĖĒÅēņāüĒö╝ņäĖĒżņĢö ĒÖśņ×ÉņØś ņ£ä ņäĖĻĘĀņ┤ØņŚÉ ClostridialesĻ│╝ ErysipelotrichalesĻ░Ć ļ¦ÄņĢśļŗż[15]. ļśÉĒĢ£ ņŗØļÅäĒÄĖĒÅēņāüĒö╝ ņĢö ņĪ░ņ¦üņŚÉņä£ Streptococcus ļ░Å PrevotellaĻ░Ć ņ”ØĻ░ĆĒĢśļŖö Ļ▓āņØĆ ļéśņü£ ņśłĒøä ņØĖņ×ÉņÖĆ ņŚ░Ļ┤ĆļÉśņŚłļŗż[16].
3. ņ£ä ņäĖĻĘĀņ┤ØĻ│╝ ņ£äņĢö
ņ£äļŖö ļé«ņØĆ ņé░ļÅäņÖĆ ļŗżņ¢æĒĢ£ ņåīĒÖö ĒÜ©ņåīĻ░Ć ņĪ┤ņ×¼ĒĢśļŖö ĒÖśĻ▓Į ļĢīļ¼ĖņŚÉ Ļ│╝Ļ▒░ņŚÉļŖö ĻĘĀņØ┤ ņāØņĪ┤ĒĢśĻĖ░ ņ¢┤ļĀżņÜ┤ Ļ││ņ£╝ļĪ£ ņŚ¼Ļ▓©ņĪīņ£╝ļéś H. pyloriĻ░Ć ļ░£Ļ▓¼ļÉśļ®┤ņä£ ĻĘĀņØ┤ ņĪ┤ņ×¼ĒĢĀ ņłś ņ׳ļŗżļŖö ņé¼ņŗżņØ┤ ļ░ØĒśĆņĪīļŗż. ĻĘĖļ¤¼ļéś ņĢäņ¦üĻ╣īņ¦Ć ļīĆļ│ĆņØä ņØ┤ņÜ®ĒĢ£ ļīĆņן ņäĖĻĘĀņ┤Ø ņŚ░ĻĄ¼ņŚÉ ļ╣äĒĢśņŚ¼ ņ£ä ņäĖĻĘĀņ┤ØņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļōżņØĆ ļ¦Äņ¦Ć ņĢŖļŗż. ņ£ä ņäĖĻĘĀņ┤ØņØĆ ĻĄ¼Ļ░ĢņØ┤ļéś ņŗØļÅä ĻĘĖļ”¼Ļ│Ā ņåīņןĻ│╝ļŖö ļŗżļźĖ ņĪ░ņä▒ņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗż. ņ£ä ņäĖĻĘĀņ┤ØņØś ņĪ░ņä▒ņŚÉļŖö H. pylori ņ£Āļ¼┤Ļ░Ć Ļ░Ćņן Ļ▓░ņĀĢņĀüņØĖ ņÜöņØĖņ£╝ļĪ£ ņ×æņÜ®ĒĢśļ®░, H. pyloriĻ░Ć ņŚåļŖö Ļ▓ĮņÜ░ņŚÉļŖö ļŗżņ¢æĒĢ£ ĻĘĀļōżņØ┤ ņ£ä ļé┤ņŚÉ ņĪ┤ņ×¼ĒĢ£ļŗż. ļČüļ»Ė ņøÉņŻ╝ļ»╝ņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö H. pyloriĻ░Ć ņØīņä▒ņØĖ Ļ▓ĮņÜ░ ActinobacteriaņÖĆ FirmicutesĻ░Ć ļŹö ņÜ░ņäĖĒĢśņśĆĻ│Ā, H. pyloriĻ░Ć ņ¢æņä▒ņØĖ Ļ▓ĮņÜ░ non-H. pylori ProteobacteriaņÖĆ AcidobacteriaĻ░Ć ņÜ░ņäĖĒĢśņśĆļŗż[17]. ĻĘĖļ¤¼ļéś H. pylori Ļ░ÉņŚ╝ ņ£Āļ¼┤Ļ░Ć ņ£ä ņäĖĻĘĀņ┤ØņŚÉ ņśüĒ¢źņØä ņŻ╝ņ¦Ć ņĢŖļŖöļŗżļŖö ņŚ░ĻĄ¼ļÅä ņ׳ļŗż[18]. H. pylori ņ£Āļ¼┤ņŚÉ Ļ┤ĆĻ│äņŚåņØ┤ Proteobacteria, Firmicutes, Actinobacteria, Bacteroidetes ļ░Å FusobacteriaĻ░Ć ņ£ä ļé┤ņŚÉ ņĪ┤ņ×¼ĒĢśļŖö ņŻ╝ņÜö ļ¼Ė(phylum)ņØ┤ļŗż[17,18]. ĒĢśņ£ä ņłśņżĆņŚÉņä£ļŖö Ļ▓Ćņé¼ ļ░®ļ▓ĢĻ│╝ ļīĆņāüņŚÉ ļö░ļØ╝ ļŗżņ¢æĒĢ£ ĻĘĀļōżņØś ņĪ┤ņ×¼ļź╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ļŖöļŹ░[19], ņśłļź╝ ļōżļ®┤ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņåŹ(genus) ņłśņżĆ ņŚ░ĻĄ¼ņŚÉņä£ļŖö Propionibacterium, Lactobacillus, Streptococcus ļ░Å StaphylococcusĻ░Ć ņŻ╝ļÉ£ ĻĘĀņŻ╝ņśĆļŗż[20]. ņ£äņĢö ļ░£ņāØņŚÉ H. pyloriĻ░Ć Ļ░Ćņן ņżæņÜöĒĢ£ ņÜöņØĖņØ┤ļØ╝ļŖö Ļ▓āņØĆ ņØśņŗ¼ĒĢĀ ļ░ö ņŚåņ£╝ļéś ļ¦īņä▒ ņ£äņŚ╝, ņןņāüĒö╝ĒÖöņāØ, ņ£äņĢöņŚÉņä£ Ļ░üĻ░ü ņ£ä ņäĖĻĘĀņ┤ØņØ┤ ņä£ļĪ£ ļŗżļź┤ļŗżļŖö Ļ▓āņØ┤ ĻĄŁļé┤ ļ░Å ņÖĖĻĄŁņØś ĒÖśņ×ÉņŚÉņä£ ļ│┤Ļ│ĀļÉśņŚłļŗż[21-23]. ĻĄŁļé┤ ĒÖśņ×ÉļōżņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņ£äņĢö ĒÖśņ×ÉņØś ņ£äņŚÉņä£ ņ£äņŚ╝ņØ┤ļéś ņןņāüĒö╝ĒÖöņāØ ĒÖśņ×ÉņŚÉ ļ╣äĒĢśņŚ¼ Bacillus Ļ░Ģ(class)Ļ│╝ Streptococcaceae Ļ│╝(family)Ļ░Ć ņ”ØĻ░ĆĒĢśņśĆļŗż[22]. Ēżļź┤Ēł¼Ļ░ł ņ£äņĢö ĒÖśņ×ÉņŚÉņä£ļŖö ņ£äņŚ╝ ĒÖśņ×ÉņŚÉ ļ╣äĒĢśņŚ¼ H. pyloriĻ░Ć Ļ░ÉņåīĒĢśļ®┤ņä£ ņāüļīĆņĀüņ£╝ļĪ£ Phyllobacterium, Achromobacter ņåŹņØ┤ļéś Xanthomonadaceae ļ░Å Enterobacteriaceae Ļ│╝Ļ░Ć ĒżĒĢ©ļÉ£ Proteobacteria ļ¼ĖņØ┤ ņ”ØĻ░ĆļÉśņŚłļŗż[21]. ļśÉ ņ£äņĢöņŚÉņä£ļŖö ņĀĢņāüņØ┤ļéś ņ£äņŚ╝ņŚÉ ļ╣äĒĢśņŚ¼ ņ£ä ņäĖĻĘĀņ┤Ø ļČłĻĘĀĒśĢņØ┤ ņŗ¼ĒĢśņśĆĻ│Ā[21-23] ļ®öĒāĆĻ▓īļåł ĻĖ░ļŖź ļČäņäØņŚÉņä£ļÅä ņ¦łņé░ņŚ╝ ĒÖśņøÉĒÜ©ņåī(nitrate reductase)ņÖĆ ņĢäņ¦łņé░ņŚ╝ ĒÖśņøÉĒÜ©ņåī(nitrite reductase) ĻĖ░ļŖźņØ┤ ņ”ØĻ░ĆļÉśņ¢┤ ņ׳ņŚłļŗż[21]. ņ£äņĢö ĒÖśņ×ÉņŚÉņä£ H. pylori ņØ┤ņÖĖņŚÉ ņ”ØĻ░ĆĒĢ£ ļŗżļźĖ ĻĘĀļōżņØ┤ ļ░£ņĢö Ļ│╝ņĀĢņŚÉ ņ¢┤ļ¢ż ņŚŁĒĢĀņØä ĒĢśļŖöņ¦Ć ņĢäņ¦ü ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśĻĖ░ ļĢīļ¼ĖņŚÉ Ē¢źĒøä ĻĖ░ņĀä ņŚ░ĻĄ¼Ļ░Ć ļŹö ņØ┤ļŻ©ņ¢┤ņĀĖņĢ╝ ĒĢ£ļŗż.
4. H. pylori ņĀ£ĻĘĀņŚÉņä£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņØś ņŚŁĒĢĀ
H. pyloriļŖö ņ£äņČĢņä▒ ņ£äņŚ╝, ņåīĒÖöņä▒ ĻČżņ¢æĻ│╝ Ļ░ÖņØĆ ņ¢æņä▒ ņ¦łĒÖś ļ░Å ņ£äņĢöņØ┤ļéś ļ│ĆņŚ░ļČĆ B ņäĖĒż ļ”╝Ēöäņóģ(mucosa-associated lymphoid tissue type)Ļ│╝ Ļ░ÖņØĆ ņĢģņä▒ ņ¦łĒÖśņØś ņøÉņØĖņØ┤ ļÉĀ ņłś ņ׳ļŗż. ĻĘĖļ¤¼ļ»ĆļĪ£ ņØ┤ņÖĆ ņŚ░Ļ┤ĆļÉ£ ņ¦łĒÖśļōżņØś ņ╣śļŻī ļ░Å ņśłļ░®ņØä ņ£äĒĢśņŚ¼ H. pylori ņĀ£ĻĘĀ ņ╣śļŻīĻ░Ć ļ¦żņÜ░ ņżæņÜöĒĢśļŗż. ĻĄŁļé┤ņŚÉņä£ļŖö ņ¢æņä▒ņ×ÉĒÄīĒöäņ¢ĄņĀ£ņĀ£, amoxicillin, clarithromycinņØä Ļ░ÖņØ┤ ņé¼ņÜ®ĒĢśļŖö ņé╝ņĀ£ņÜöļ▓ĢņØ┤ 1ņ░© ņ╣śļŻīļĪ£ ņé¼ņÜ®ļÉśĻ│Ā ņ׳ņ¦Ćļ¦ī ņĀ£ĻĘĀņ£©ņØ┤ ņĀÉņ░©ņĀüņ£╝ļĪ£ Ļ░ÉņåīĒĢśļŖö Ļ▓āņØ┤ ļ¼ĖņĀ£Ļ░Ć ļÉśĻ│Ā ņ׳ļŗż[24]. ņØ┤ļ¤¼ĒĢ£ ņĀ£ĻĘĀ ņŗżĒī©ņØś ņŻ╝ņÜö ņøÉņØĖņØĆ ĒĢŁņāØņĀ£ ļé┤ņä▒ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ H. pylori ņĀ£ĻĘĀņ£©ņØä Ē¢źņāüņŗ£ĒéżĻĖ░ ņ£äĒĢśņŚ¼ Ļ░ĢļĀźĒĢ£ ņ£äņé░ ņ¢ĄņĀ£ņĀ£ņØś ņé¼ņÜ®, ņł£ņ░© ņ╣śļŻī, ļÅÖņŗ£ ņ╣śļŻī, ņāłļĪ£ņÜ┤ ĒĢŁņāØņĀ£ņØś ņé¼ņÜ® ļō▒ņØś ņĀäļץņØ┤ ņŗ£ļÅäļÉśĻ│Ā ņ׳ļŗż. ņØ┤ļ¤¼ĒĢ£ ļģĖļĀźņØś ņØ╝ĒÖśņ£╝ļĪ£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżļź╝ ņĀ£ĻĘĀ ņ╣śļŻīņÖĆ ĒĢ©Ļ╗ś ņé¼ņÜ®ĒĢ┤ ņÖöņ£╝ļ®░, ĻĘĖ ĻĖ░ņĀäņØĆ H. pyloriņŚÉ ļīĆĒĢ£ ņ¦üņĀæ ņ¢ĄņĀ£ ĒÜ©Ļ│╝, ņĀÉļ¦ē ļ░®ņ¢┤ Ļ░ĢĒÖö ĒÜ©Ļ│╝, ļ®┤ņŚŁ ļ░śņØæ ņĪ░ņĀł ĒÜ©Ļ│╝, IgA ļČäļ╣ä ļō▒Ļ│╝ ĒĢ©Ļ╗ś ĒĢŁņāØņĀ£ ņé¼ņÜ®Ļ│╝ ņŚ░Ļ┤ĆļÉ£ ļČĆņ×æņÜ®ņØä Ļ░Éņåīņŗ£ņ╝£ ņĢĮņĀ£ ļ│ĄņÜ® ņł£ņØæļÅäļź╝ ļåÆņØ┤ļŖö Ļ▓ā ļō▒ņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[25,26]. ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖż ļŗ©ļÅģ Ēł¼ņŚ¼ļŖö H. pylori ĒÖ£ņä▒ņØä ļé«ņČ£ ņłśļŖö ņ׳ņ£╝ļéś ņĀ£ĻĘĀņØä ņŗ£Ēéżņ¦ĆļŖö ļ¬╗ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ Ēæ£ņżĆ ņé╝ņĀ£ņÜöļ▓ĢņØä ĻĖ░ļ│Ėņ£╝ļĪ£ ĒĢśĻ│Ā ņČöĻ░ĆļĪ£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżļź╝ Ēł¼ņŚ¼ĒĢśĻ▓ī ļÉśļŖöļŹ░, ņØ┤ļ¤░ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖż ņČöĻ░Ć Ēł¼ņŚ¼Ļ░Ć ņĀ£ĻĘĀņ£©ņØä Ē¢źņāüņŗ£ĒéżļŖöņ¦Ć ĻŠĖņżĆĒ׳ ņŚ░ĻĄ¼ļÉśĻ│Ā ņ׳ļŗż[27]. ņĄ£ĻĘ╝ 3ļģä ļÅÖņĢł ļ░£Ēæ£ļÉ£ 7Ļ░£ņØś ļ®öĒāĆļČäņäØ ļ¬©ļæÉ ņĀ£ĻĘĀ ņ╣śļŻīņÜöļ▓ĢņŚÉ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżļź╝ ņČöĻ░ĆĒĢśļŖö Ļ▓ĮņÜ░ ņĀ£ĻĘĀņ£©ņØä Ļ░£ņäĀņŗ£ņ╝░ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż(relative risk [RR], 1.12~1.85) (Table 1) [25,28-38]. ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖż ņČöĻ░Ć Ēł¼ņŚ¼ņØś ņżæņÜöĒĢ£ ĒÜ©Ļ│╝ļŖö ĒĢŁņāØņĀ£ņÖĆ ņŚ░Ļ┤ĆļÉ£ ļČĆņ×æņÜ®ņØä Ļ░Éņåī(RR, 0.40~0.45)ņŗ£ņ╝£ ņĢĮņĀ£ ļ│ĄņÜ® ņł£ņØæļÅäļź╝ ļåÆņØ╝ ņłś ņ׳ļŗżļŖö Ļ▓āņØĖļŹ░, ĒŖ╣Ē׳ ņäżņé¼ ņ”ØņāüņØĆ ļīĆļČĆļČäņØś ņŚ░ĻĄ¼ņŚÉņä£ Ļ░ÉņåīļÉśņŚłļŗż(RR, 0.3~0.54). ĒĢ£ ļ®öĒāĆļČäņäØņŚÉņä£ļŖö Ēæ£ņżĆ ņé╝ņĀ£ņÜöļ▓ĢņŚÉ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖż ļ│ĄĒĢ® ĻĘĀņŻ╝ļź╝ Ļ░ÖņØ┤ ņé¼ņÜ®ĒĢ£ Ļ▓ĮņÜ░ H. pylori ņĀ£ĻĘĀ ņä▒Ļ│ĄņŚÉ ļīĆĒĢ£ number needed to treatļŖö 10.2ņśĆĻ│Ā, ĒĢŁņāØņĀ£ ņŚ░Ļ┤Ć ļČĆņ×æņÜ®ņØä ņĢĮ 14% ņĀĢļÅä Ļ░Éņåīņŗ£ņ╝░ļŗż[32]. Ēśäņ×¼Ļ╣īņ¦ĆņØś ņŚ░ĻĄ¼ļōżņØä ņóģĒĢ®ĒĢ┤ļ│┤ļ®┤ ļŗżņ¢æĒĢ£ ņóģļźśņØś ļŗ©ņØ╝ Ēś╣ņØĆ ļ│ĄĒĢ® ĻĘĀņŻ╝ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżĻ░Ć ļÅÖņ¢æ ļ░Å ņä£ņ¢æņØś ņŚ░ĻĄ¼ ļ¬©ļæÉņŚÉņä£ ņĀ£ĻĘĀņ£©ņØä ņ”ØĻ░Ćņŗ£ĒéżĻ│Ā ĒĢŁņāØņĀ£ ņŚ░Ļ┤Ć ņäżņé¼ļź╝ Ļ░Éņåīņŗ£ņ╝░ņ¦Ćļ¦ī ĻĘĖ ĒÜ©Ļ│╝ļŖö Ēü¼ņ¦Ć ņĢŖņĢśļŗż[25].
5. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ ņ£ä ņäĖĻĘĀņ┤ØņØś ņØ┤ņāüĻ│╝ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņØś ņŚŁĒĢĀ
ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØś ļ░£ņāØ ĻĖ░ņĀäņ£╝ļĪ£ ļé┤ņן Ļ│╝ļ»╝ņä▒, ņ£äļ░░ņČ£ ņןņĢĀ, ņ£äņĪ░ņĀł ņןņĢĀ ļō▒ņØ┤ ņĢīļĀżņĀĖ ņ׳ļŗż. ņĄ£ĻĘ╝ ĻĖ░ļŖźņä▒ ņ£äņןĻ┤Ć ņ¦łĒÖśņŚÉņä£ ņןļé┤ ņäĖĻĘĀņØś ņŚŁĒĢĀņØ┤ Ļ░ĢņĪ░ļÉśļ®┤ņä£ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņØś ņ£ä ņäĖĻĘĀņ┤Ø ļ│ĆĒÖöļź╝ Ļ┤Ćņ░░ĒĢ£ ņåīĻĘ£ļ¬© ņŚ░ĻĄ¼ļōżņØ┤ ņŗ£Ē¢ēļÉśņŚłļŗż. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×Éļź╝ ļīĆņāüņ£╝ļĪ£ terminal restriction fragment length polymorphismņØä ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ Bifidobacterium ņ”ØĻ░Ć, Prevotella Ļ░Éņåī, Clostridium IX, XI, XVIII ņ”ØĻ░ĆņÖĆ Ļ░ÖņØĆ ņ£ä ņäĖĻĘĀņ┤Ø ņØ┤ņāüņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā[3], ņ░©ņäĖļīĆ ņŚ╝ĻĖ░ ļČäņäØ ļ░®ļ▓ĢņØä ņØ┤ņÜ®ĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö Bacteriodetes ņ”ØĻ░Ć, Proteobacteria Ļ░Éņåī, Acidobacteria Ļ░ÉņåīĻ░Ć Ļ┤Ćņ░░ļÉśņŚłļŗż. ņåŹ ņłśņżĆņŚÉņä£ļŖö Bacteroides ņ”ØĻ░ĆņÖĆ Edaphobacter Ļ░ÉņåīĻ░Ć Ļ┤Ćņ░░ļÉśņŚłĻ│Ā ņóģ(species) ņłśņżĆņŚÉņä£ļŖö Bacteriodes dorei ļ░Å Escherichia coli/shigella ņ”ØĻ░Ć ĻĘĖļ”¼Ļ│Ā Edaphobacter aggregans Ļ░ÉņåīĻ░Ć Ļ┤Ćņ░░ļÉśņŚłļŗż. ĒØźļ»ĖļĪŁĻ▓īļÅä ņØ┤ļ¤¼ĒĢ£ ņ£ä ņäĖĻĘĀņ┤ØņØś ņØ┤ņāüņØĆ Lactobacillus gasseri OLL2716 ņÜöĻ▒░ĒŖĖļź╝ Ēł¼ņŚ¼ĒĢśņśĆņØä ļĢī ņĀĢņāüņØĖĻ│╝ ļ╣äņŖĘĒĢśĻ▓ī ĒÜīļ│ĄļÉśņŚłļŗż[39]. ņĄ£ĻĘ╝ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżĻ░Ć ĒśĖņĀäņŗ£Ēé¼ ņłś ņ׳ļŖöņ¦ĆņŚÉ ļīĆĒĢśņŚ¼ ņåīĻĘ£ļ¬© ņŚ░ĻĄ¼Ļ░Ć ļ░£Ēæ£ļÉśņŚłļŗż. H. pylori Ļ░ÉņŚ╝ņØ┤ ņŚåļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉĻ▓ī Lactobacillus gasseri OLL2716 ņÜöĻ▒░ĒŖĖļź╝ Ēł¼ņŚ¼ĒĢśļ®┤ 12ņŻ╝ņ¦ĖņŚÉ ņ£ĀņØśĒĢśĻ▓ī ņ£äņĢĮļ│┤ļŗż ņ”Øņāü ĒśĖņĀäņ£©ņØ┤ ļåÆņĢśļŗż. ņŗØĒøä ĒīĮļ¦īĻ░É, ņĪ░ĻĖ░ Ēżļ¦īĻ░É ļō▒ ņŗØĒøä ļČłĒÄĖ ņ”ØĒøäĻĄ░(postprandial distress syndrome) ņ”ØņāüņØä ĒśĖņĀäņŗ£ņ╝░ņ£╝ļéś ņāüļ│ĄļČĆ ĒåĄņ”ØĻ│╝ ņåŹņō░ļ”╝ņØĆ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż[40,41]. Bifidobacterium bifidum YIT 10347 ļ░£ĒÜ©ņ£Āļź╝ 4ņŻ╝Ļ░ä ļ│ĄņÜ®ĒĢ£ ļæÉ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņåīĒÖöļČłļ¤ē, ņ£äņé░Ļ│╝ ņŚ░Ļ┤ĆļÉ£ ņ”Øņāü, ņŗØĒøä ļČłĒÄĖĻ░ÉĻ│╝ ņāüļ│ĄļČĆ ĒåĄņ”ØņØ┤ ĒśĖņĀäļÉśņŚłņØä ļ┐Éļ¦ī ņĢäļŗłļØ╝ ņĀĢņŗĀņĀüņØĖ ņ”ØņāüļÅä Ļ░ÖņØ┤ ĒśĖņĀäļÉśņŚłļŗż[42,43]. ņżæļ»Ė ņ¦ĆņŚŁņŚÉņä£ ņłśĒ¢ēļÉ£ ņŚ░ĻĄ¼ņŚÉņä£ Bacillus coagulans ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżļź╝ ĒÖśņ×ÉņŚÉĻ▓ī Ēł¼ņŚ¼ĒĢśļ®┤ ņ£äņןĻ┤Ć ņ”Øņāü ņĀÉņłśņØś ņ┤ØņĀÉĻ│╝ ļ│ĄĒåĄ ņĀÉņłśĻ░Ć ĒśĖņĀäļÉśņŚłļŗż[44]. ĻĘĖļ¤¼ļéś Bifidobacterium bifidum YIT 10347ņÖĆ Bacillus coagulans ņŚ░ĻĄ¼ļŖö ļīĆņāü ĒÖśņ×ÉĻĄ░ņØ┤ Rome ĻĖ░ņżĆņØä ļ¦īņĪ▒ĒĢśņ¦Ć ļ¬╗ĒĢśĻ│Ā ņåīĒÖöļČłļ¤ē ņ”ØņāüņØä ņØ╝ņŗ£ņĀüņ£╝ļĪ£ Ļ░Ćņ¦ä ĒÖśņ×ÉļōżņØ┤ņŚłļŗżļŖö ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ņŚłļŗż. ņØ┤Ēāłļ”¼ņĢäņØś ņŚ░ĻĄ¼ņŚÉņä£ļŖö ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”Ø ĒÖśņ×ÉņŚÉĻ▓ī ņś¼ļ”¼ļĖīņ£ĀņÖĆ ĒĢ©Ļ╗ś Lactobacillus reuteri, Lactobacillus rhamnosus GG ļ░Å Saccharomyces boulardiiĻ░Ć ĒżĒĢ©ļÉ£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżļź╝ 7ņØ╝Ļ░ä Ēł¼ņŚ¼ĒĢ£ Ļ▓ĮņÜ░ ņś¼ļ”¼ļĖīņ£Ā ļŗ©ļÅģ Ēł¼ņŚ¼ļéś ņś¼ļ”¼ļĖīņ£ĀņÖĆ ĒĢŁņé░ĒÖöņĀ£ļź╝ Ļ░ÖņØ┤ Ēł¼ņŚ¼ĒĢ£ Ļ▓ĮņÜ░ņŚÉ ļ╣äĒĢśņŚ¼ ņ£ĀņØśĒĢśĻ▓ī ņśżņŗ¼, ņāüļ│ĄļČĆ ĒåĄņ”Ø, ņŗØĒøä ĒīĮļ¦ī, ĒŖĖļ”╝ ļō▒ņØś ņ”ØņāüņØ┤ ĒśĖņĀäļÉśņŚłļŗż[45].
6. NSAIDņŚÉ ņØśĒĢ£ ņåīņן ņĀÉļ¦ēņåÉņāü ĻĖ░ņĀäņŚÉņä£ ņןļé┤ ņäĖĻĘĀņ┤ØņØś ņŚŁĒĢĀ
ļīĆņןņØ┤ļéś ņ£äņŚÉ ļ╣äĒĢśņŚ¼ ņåīņןņØĆ ņĀæĻĘ╝ņØ┤ ļ¦żņÜ░ ņ¢┤ļĀĄĻĖ░ ļĢīļ¼ĖņŚÉ ņØĖĻ░äņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ ņåīņן ņäĖĻĘĀņ┤Ø ņŚ░ĻĄ¼ļŖö ĒÜīņןņĪ░ļŻ©ņłĀ ĒÖśņ×ÉņŚÉņä£ ņŗ£Ē¢ēļÉ£ Ļ▓ā ņÖĖņŚÉ Ļ▒░ņØś ņŚåļŗż. ļ╣äĻĄÉņĀü ņĢłņĀĢņĀüņØĖ ļīĆņן ņäĖĻĘĀņ┤ØņŚÉ ļ╣äĒĢśņŚ¼ ņåīņן ņäĖĻĘĀņ┤ØņØĆ ņØīņŗØ ņäŁņĘ©ņŚÉ ļö░ļØ╝ ņ¦¦ņØĆ ņŗ£Ļ░ä ļé┤ņŚÉ ņĪ░ņä▒ņØ┤ ļ░öļĆö ņłś ņ׳ļŗż. ņØĖĻ░ä ļīĆņāü ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņåīņןņŚÉņä£ StreptococcusņÖĆ VeillonellaĻ░Ć ļ╣äĻĄÉņĀü ņØ╝Ļ┤ĆļÉśĻ▓ī Ļ┤Ćņ░░ļÉśļ®░ Clostridium, Escherichia ļ░Å TuricibacterļŖö ļŗżņ¢æĒĢ£ ļ╣łļÅäļĪ£ ņĪ┤ņ×¼ĒĢ£ļŗż[46]. ņ¦üņĀæ ņןņØä ņĀüņČ£ĒĢśņŚ¼ ņäĖĻĘĀņ┤ØņØä ņĪ░ņé¼ĒĢĀ ņłś ņ׳ļŖö ņāØņźÉ(mice) ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņåīņןņŚÉ ņŻ╝ļĪ£ LactobacillaceaeĻ░Ć ņĪ┤ņ×¼ĒĢśļŖö Ļ▓āņØ┤ ĒÖĢņØĖļÉśņŚłļŗż[47]. ņåīņן ļé┤ ņäĖĻĘĀņ┤ØņØĆ ņØīņŗØņ£╝ļĪ£ ņäŁņĘ©ļÉ£ ļŗ©ļŗ╣ļźśļź╝ ļīĆņé¼ņŗ£ņ╝£ ļŗ©ņćäņ¦Ćļ░®ņé░ņØä ņāØņé░ĒĢśĻ│Ā ļŗżņ¢æĒĢ£ ļ®┤ņŚŁ ļ░śņØæņØä ņØ╝ņ£╝ĒéżļŖö ņŚŁĒĢĀņØä ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤ņØĖļŗż[46].
NSAIDļŖö H. pyloriņÖĆ ĒĢ©Ļ╗ś ņåīĒÖöņä▒ ĻČżņ¢æņØś Ļ░Ćņן ņżæņÜöĒĢ£ ņøÉņØĖ ņżæ ĒĢśļéśņØĖļŹ░, ņ£äņÖĆ ņŗŁņØ┤ņ¦Ćņן ņÖĖņŚÉļÅä ņåīņן ņĀÉļ¦ē ņåÉņāüņØä ņØ╝ņ£╝ņ╝£ ļ│ĄĒåĄņØ┤ļéś ņČ£ĒśłņØś ņøÉņØĖņØ┤ ļÉśĻĖ░ļÅä ĒĢ£ļŗż. NSAID Ēł¼ņŚ¼ļĪ£ ņåīņן ņĀÉļ¦ē ņåÉņāüņØ┤ ņØ╝ņ¢┤ļéśļŖö Ļ│╝ņĀĢņŚÉ ņןļé┤ ņäĖĻĘĀņØ┤ ņŚ░Ļ┤ĆļÉ£ļŗżļŖö Ļ▓āņØĆ ņśżļל ņĀäļČĆĒä░ ņĢīļĀżņĪīļŗż. ņĢĮ 40ļģä ņĀäņŚÉ ņŗ£Ē¢ēļÉ£ ņŚ░ĻĄ¼ņŚÉņä£ ņĀĢņāü ņןļé┤ ņäĖĻĘĀņ┤ØņØä Ļ░Ćņ¦ä ņźÉņŚÉ ļ╣äĒĢśņŚ¼ ļ¼┤ĻĘĀņźÉņŚÉņä£ļŖö indomethacin Ēł¼ņŚ¼ ĒøäņŚÉļÅä ņåīņן ņĀÉļ¦ē ņåÉņāüņØ┤ Ļ▓Įļ»ĖĒ¢łņ£╝ļ®░, ĒŖ╣Ē׳ ņłśņ╗Ę ļ¼┤ĻĘĀņźÉņŚÉņä£ļŖö ņĀÉļ¦ē ņåÉņāüņØ┤ ļ░£ņāØĒĢśņ¦Ć ņĢŖņĢśļŗż[48]. ĒøäņåŹ ņŚ░ĻĄ¼ņŚÉņä£ ļ¼┤ĻĘĀņźÉņŚÉ Escherichia coliļéś EubacteriumņØä ņØ┤ņŗØĒĢśĻ│Ā NSAIDļź╝ Ēł¼ņŚ¼ĒĢśļ®┤ ņåīņן ņĀÉļ¦ē ņåÉņāüņØ┤ ļ░£ņāØĒĢśņ¦Ćļ¦ī ĒĢŁņāØņĀ£ļź╝ Ļ░ÖņØ┤ Ēł¼ņŚ¼ĒĢśļ®┤ ļ░£ņāØĒĢśņ¦Ć ņĢŖņĢśĻ│Ā, BifidobacteriumņØ┤ļéś Lactobacillusļź╝ ņØ┤ņŗØĒĢśļŖö Ļ▓ĮņÜ░ņŚÉļÅä NSAID ņ£Āļ░£ ņåīņן ņĀÉļ¦ē ņåÉņāüņØ┤ ļ░£ņāØĒĢśņ¦Ć ņĢŖņĢśļŗż[49]. ņØ┤ļĀćĻ▓ī NSAID ņ£Āļ░£ ņåīņן ņĀÉļ¦ē ņåÉņāü ļ░£ņāØ Ļ│╝ņĀĢņŚÉ ĒŖ╣ņĀĢ ņןļé┤ ņäĖĻĘĀņØ┤ ņŚ░Ļ┤ĆļÉ£ļŗżļŖö Ļ▓░Ļ│╝ļŖö ņåīņן ņĀÉļ¦ē ņåÉņāüņØś Ļ▓ĮņÜ░ ņ£ä ņĀÉļ¦ē ņåÉņāüĻ│╝ļŖö ļŗżļźĖ ĻĖ░ņĀäņØ┤ ņ×æņÜ®ĒĢ£ļŗżļŖö Ļ▓āņØä ņŗ£ņé¼ĒĢ£ļŗż. ņ”ē NSAIDĻ░Ć prostaglandinņØä Ļ░Éņåīņŗ£ņ╝£ ņåīņן ņĀÉļ¦ēņØś ļ░®ņ¢┤ ĻĖ░ļŖźĻ│╝ Ēł¼Ļ│╝ļÅäņŚÉ ņØ┤ņāüņØ┤ ņāØĻĖ░ļ®┤ ņןļé┤ ņäĖĻĘĀņØ┤ļéś lipopolysaccharideņÖĆ Ļ░ÖņØĆ ņŚ╝ņ”Ø ņ£Āļ░£ ļ¼╝ņ¦łņØś ņĀÉļ¦ē ņ╣©Ēł¼Ļ░Ć ļ░£ņāØĒĢśĻ│Ā, ņØ┤ļĪ£ ņØĖĒĢśņŚ¼ ņĀÉļ¦ēĒĢśņŚÉņä£ tumor necrosis factor-╬▒, interleukin-1╬▓ ņ”ØĻ░ĆņÖĆ Ļ░ÖņØĆ ņŚ╝ņ”Ø ļ░śņØæņØ┤ ņØ╝ņ¢┤ļéś ņåīņן ņĀÉļ¦ēņäĖĒżļź╝ ņåÉņāüņŗ£ĒéżļŖö Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉśĻ│Ā ņ׳ļŗż[5]. Toll-like receptor 4ļéś myeloid differentiation primary-response 88 Ļ▓░ņåÉ ņāØņźÉ(knock out mice)ņŚÉņä£ļŖö NSAIDņŚÉ ņØśĒĢ£ ņåīņן ņĀÉļ¦ē ņåÉņāüņØ┤ ņĢĮĒĢśĻ▓ī ļéśĒāĆļéśĻĖ░ ļĢīļ¼ĖņŚÉ NSAID ņ£Āļ░£ ņåīņן ņĀÉļ¦ē ņåÉņāü Ļ│╝ņĀĢņØĆ toll-like receptor 4ņŚÉ ņØśņĪ┤ņĀüņØĖ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[50]. NSAID ņ£Āļ░£ ņåīņן ņĀÉļ¦ē ņåÉņāüņŚÉ ļīĆĒĢ£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņØś ĒÜ©Ļ│╝ļź╝ ĒÖĢņØĖĒĢ£ ņŚ░ĻĄ¼ļŖö ļ¦żņÜ░ ņĀüņØĆļŹ░, Lactobacillus casei ĻĘĀņŻ╝ļŖö ļÅÖļ¼╝ ņŗżĒŚśņŚÉņä£ ņĀÉļ¦ē ņåÉņāüņØä ņżäņśĆņØäļ┐Éļ¦ī ņĢäļŗłļØ╝ ņØĖĻ░ä ļīĆņāü ņŚ░ĻĄ¼ņŚÉņä£ļÅä ņåīņן ņ║ĪņŖÉļé┤ņŗ£Ļ▓ĮņŚÉņä£ ņĀÉļ¦ē ņåÉņāü ņĀÉņłśļź╝ ļé«ņČöņŚłļŗż[51,52]. ļśÉĒĢ£ ļ│ĄĒĢ® ĻĘĀņŻ╝ņØĖ VSL#3 ļ│ĄņÜ®ņØĆ ļ│ĄņÜ®ĒĢśņ¦Ć ņĢŖņØĆ ļīĆņĪ░ĻĄ░ņŚÉ ļ╣äĒĢśņŚ¼ NSAID Ēł¼ņŚ¼ Ēøä ļīĆļ│Ć calprotectin ņ¢æņØä ļŹö ļé«ņČöņŚłļŗż[53].
Ļ▓░ ļĪĀ
ņĢäņ¦üĻ╣īņ¦Ć ļīĆņן ņ¦łĒÖśņØ┤ļéś ļīĆņé¼ ņ¦łĒÖśņŚÉ ļ╣äĒĢśņŚ¼ ņāüļČĆņ£äņןĻ┤Ć ņ¦łĒÖśņŚÉņä£ļŖö ņןļé┤ ņäĖĻĘĀņ┤ØņØś ņŚŁĒĢĀņØ┤ ņל ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśļŗż. ļ░öļĀøņŗØļÅä, ņŗØļÅäņäĀņĢö, ņ£äņĢöĻ│╝ ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņŚÉņä£ļŖö ņØ╝ļČĆ ņŚŁĒĢĀņØä ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤ņØ┤Ļ│Ā NSAIDņŚÉ ņØśĒĢ£ ņåīņן ņĀÉļ¦ē ņåÉņāü ļ░£ņāØ ĻĖ░ņĀäņŚÉļŖö ņżæņČöņĀüņØĖ ņŚŁĒĢĀņØä ĒĢ£ļŗż. ņāüļČĆņ£äņןĻ┤Ć ņ¦łĒÖśņØś ņ╣śļŻīņĀüņØĖ ņĖĪļ®┤ņŚÉņä£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖż ņé¼ņÜ®ņØĆ ņĢäņ¦ü ĻĘĖ ĒÜ©Ļ│╝Ļ░Ć ļČłļČäļ¬ģĒĢśļŗż. Ļ░Ćņן ĒØöĒ׳ ņé¼ņÜ®ļÉśļŖö Ļ▓ĮņÜ░ļŖö H. pylori ņĀ£ĻĘĀ ņÜöļ▓ĢņŚÉ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżļź╝ ņČöĻ░ĆĒĢśļŖö Ļ▓āņ£╝ļĪ£, ņäżņé¼ņÖĆ Ļ░ÖņØĆ ĒĢŁņāØņĀ£ ņŚ░Ļ┤Ć ļČĆņ×æņÜ®ņØä Ļ░Éņåīņŗ£ņ╝£ ļ│ĄņĢĮ ņł£ņØæļÅäļź╝ ļåÆņØ╝ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ĻĖ░ļŖźņä▒ ņåīĒÖöļČłļ¤ēņ”ØņØ┤ļéś NSAIDņŚÉ ņØśĒĢ£ ņåīņן ņĀÉļ¦ē ņåÉņāüņŚÉņä£ļÅä ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżĻ░Ć ņ£ĀņÜ®ĒĢĀ ņłś ņ׳ļŗżļŖö ņ”ØĻ▒░ļōżņØ┤ ņĀ£ņŗ£ļÉśņŚłņ£╝ļéś ņĢäņ¦ü ņŚ░ĻĄ¼Ļ░Ć ļČĆņĪ▒ĒĢ£ ĒÄĖņØ┤ļŗż. ļśÉĒĢ£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņØś ĒÜ©Ļ│╝ļŖö ĻĘĀņŻ╝ ĒŖ╣ņØ┤ņĀüņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ĒŖ╣ņĀĢ ĻĘĀņŻ╝ņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝ļź╝ ļ¬©ļōĀ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņŚÉ ļÅÖņØ╝ĒĢśĻ▓ī ņĀüņÜ®ĒĢĀ ņłśļŖö ņŚåļŗż. Ē¢źĒøä ņāüļČĆņ£äņןĻ┤Ć ņ¦łĒÖśņŚÉņä£ ņäĖĻĘĀņ┤ØņØś ņŚŁĒĢĀņØ┤ ļŹö ļ░ØĒśĆņ¦ĆĻ│Ā strain ņłśņżĆņŚÉņä£ ĒöäļĪ£ļ░öņØ┤ņśżĒŗ▒ņŖżņØś ņ×æņÜ® ĻĖ░ņĀäņØ┤ ļ░ØĒśĆņ¦Ćļ®┤ ņāüļČĆņ£äņןĻ┤Ć ņ¦łĒÖśņØś ņןļé┤ ņäĖĻĘĀ ĻĖ░ļ░ś ņ╣śļŻī ļ░®ļ▓Ģņ£╝ļĪ£ ņ£ĀņÜ®ĒĢśĻ▓ī ņé¼ņÜ®ļÉĀ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.