검진 내시경에서 발견된 분문부의 위암들
Gastric Cancer of the Cardia Detected on Screening Endoscopy
Article information

요약: 54세 남자 환자가 내시경 검사를 위해 방문하였다. 환자는 가끔 역류 증상이 있었으나 특별한 치료를 하지는 않았었고 고혈압으로 투약 중이었다. 환자는 1년 전에 신장암으로 좌측 신장의 부분 절제술을 받은 병력이 있었다. 일반 혈액 검사와 간기능 검사는 정상 범위였으며 신기능 역시 BUN/Cr 14/1.1 mg/dL로 정상 범위였다. CEA는 2.4 ng/mL였고 CA19-9는 <1.0 U/mL로 역시 정상이었다. 위내시경에서 처음 분문부를 관찰하였을 시에는 일견 정상으로 보이나 공기를 넣고 근접하여 보았을 때 분문부 후벽측에 6 mm 내외의 얕은 궤양이 관찰되었다(Fig. 1).
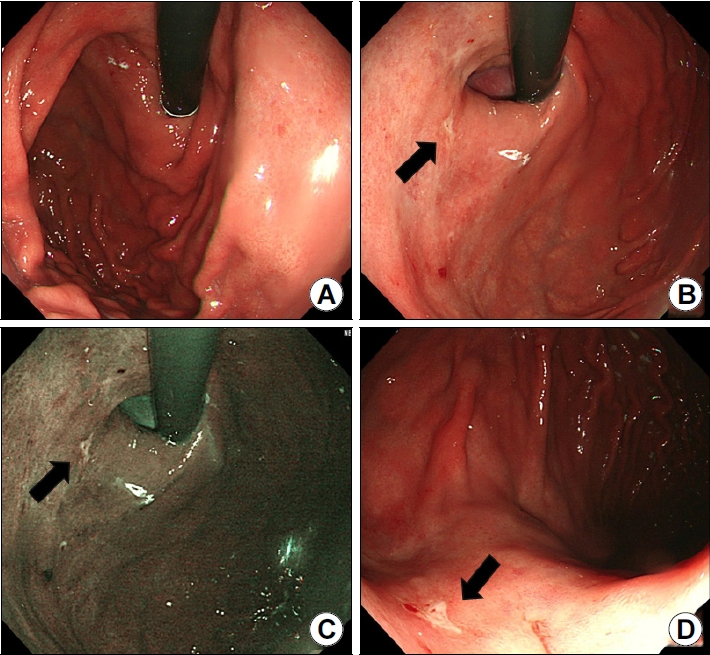
Endoscopic findings of patient 1. (A) Image showing a distant view of the cardia. The lesion is not well visualized owing to insufficient insufflation. (B) Image showing an irregularly shaped shallow ulcer involving the cardia P/W side measuring 0.6 cm in size (black arrow). (C) Lesion observed on narrow band imaging (black arrow). (D) Forward view of the lesion (black arrow).
56세 남자 환자가 내시경 검사를 위해 방문하였다. 환자는 목의 이물감 증상을 호소하고 있었고 당뇨로 투약 중이었다. 2007년에 충수돌기염과 복막염으로 수술받은 병력이 있었다. 내시경에서 분문부의 직하부 후벽 측에 1 cm가량 크기의 불규칙한 발적을 동반한 함몰된 병변이 관찰되었다(Fig. 2). 위 두 병변의 내시경 진단은 무엇이며 진단과 치료 과정에서 유의할 점들은 어떤 것들이 있는가?
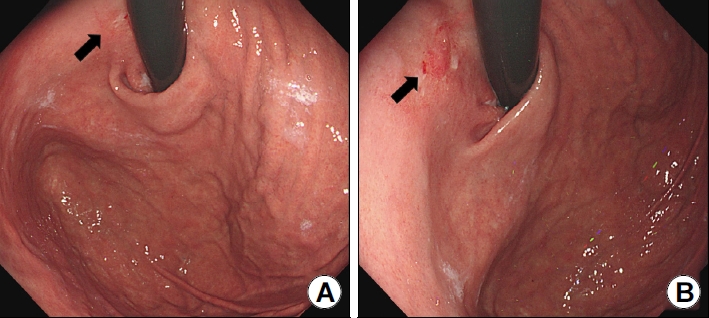
Endoscopic findings of patient 2. (A) Image showing a J-turn view of the cardia (black arrow). The lesion is not clearly visualized owing to the endoscope. (B) Image showing an irregularly shaped depressed lesion involving the cardia P/W side measuring 1.0 cm in size (black arrow).
해설: 첫 번째 환자는 조직 검사 결과 저분화 선암(adenocarcinoma, poorly differentiated)으로 진단되었다. 초음파내시경을 시행하였고 분문부 후벽 측에 29 mm 크기의 점막하 침윤이 의심되는 병변이 관찰되었으며 인근 림프절의 전이 소견은 관찰되지 않았다. 환자는 로봇을 통한 근위부 위절제술(robot-assisted proximal gastrectomy)을 받았으며, 병리 검사 결과 3.2×2.0 cm 크기의 poorly cohesive carcinoma 소견을 보였다(Fig. 3). 점막하 침윤이 관찰되었으며 침윤의 깊이는 0.7 mm로 측정이 되었고 림프절 전이는 관찰되지 않아 최종 병기는 pT1bN0로 진단되었으며 현재 추적 관찰 중이다.
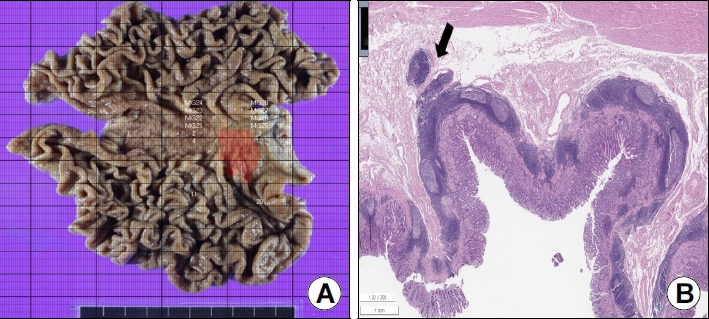
Gross morphology and histological findings of patient 1. (A) Mapped image of the surgical specimen showing the carcinoma (red). (B) Image showing carcinoma invading the submucosa (black arrow) (H&E, ×40). H&E, hematoxylin and eosin.
두 번째 환자 역시 조직 검사 결과 인환세포를 동반한 저분화 선암(adenocarcinoma, poorly differentiated with signet ring cell carcinoma component)으로 진단되었다. 초음파내시경에서는 2 cm가량 크기의 점막하 침윤이 의심되는 병변이 관찰되었으며 림프절 전이 소견은 없었다. 환자는 복강경을 통한 근위부 위절제술(laparoscopy-assissted proximal gastrectomy)을 받았고 병리 검사 결과 2.0×1.0 cm 크기의 poorly cohesive carcinoma였다(Fig. 4). 침윤은 점막근판(lamina propria)까지 있었으며 림프절 전이는 관찰되지 않아 최종 병기는 pT1aN0 였으며 이후 별 문제없이 추적 관찰 중이다.

Gross morphology and histological findings of patient 2. (A) Mapped image of the surgical specimen showing carcinoma (red). (B) Image showing carcinoma confined to the mucosa (H&E, ×40). H&E, hematoxylin and eosin.
위내시경 시에 위암, 특히 조기 위암을 놓치지 않기 위해서는 충분한 관찰 시간을 가지고 세밀하게 관찰을 하는 것이 필요하다. 국내의 연구에 의하면 3분 이상 관찰을 하는 경우에 전암성 병변이나 위암의 발견율이 유의하게 높았다는 결과가 있으며 유럽의 가이드라인에서는 4분 이상의 충분한 관찰 시간을 권고하고 있다[1,2]. 그럼에도 불구하고 해부학적 구조상 또는 내시경의 관찰 범위에 의해 맹점이 되기 쉬운 부위들이 존재하는데, 대표적으로 잘 알려진 부위들은 분문부, 체부 후벽, 유문부와 유문부 뒤쪽 부위들이다. 국내의 보고에 의하면 진행성 위암 환자 중 6개월 이내에 내시경을 받았으나 그 당시 진행성 위암으로 진단받지 못한 16명 중 6명이 분문부의 위암이었다[3]. 위 증례들에서 확인할 수 있듯이 크기가 작은 분문부의 조기 위암의 경우 불충분한 공기 주입, 환자의 구역 반응, 위내시경 기구 자체에 방해로 인해 세밀한 관찰이 이뤄지지 않은 경우 놓칠 수 있는 가능성이 있으므로 주의가 필요하다.
분문부의 선암종은 다른 부위의 위암과 달리 예후가 불량한 것으로 알려져 있는데, 그 이유로는 조기 발견이 어려워 진단 당시 진행된 상태인 경우가 많고 광범위한 림프 배출로 림프절 전이가 잘 되는 특성을 가지고 있기 때문이다[4]. 분문부의 위암이라 하더라도 I 또는 II 병기에서 발견된 경우에는 원위부 위암과 생존율에 있어서 유의한 차이를 보이지는 않았으나 III기 이후에서는 근위부 위암은 더 안 좋은 예후를 보였다[5]. 따라서 조기에만 발견된다면 비교적 좋은 예후를 보일 수 있기 때문에 내시경 시 이 부위의 세밀한 관찰은 환자의 예후에 직접적으로 영향을 줄 수 있다고 생각된다. 그리고 위 두 증례에서는 내시경에서 보이는 병변의 크기에 비해 병리에서 최종적으로 측정된 병변의 크기가 다소 큰데 이는 부위의 특징 이외에도 저분화도의 암종이었다는 점에서 기인한 것으로 보인다. 따라서 분문부에서 저분화도를 보이는 암종의 경우 치료 전에 색소내시경, 영상강화내시경, 맵핑 조직검사 등으로 병변의 범위를 정확하게 평가하고, 초음파내시경과 위 전산화단층촬영(stomach computed tomography) 등을 통해 병변의 깊이를 정확하게 평가하는 것이 치료 방침 결정에 필요할 것으로 생각된다.
Notes
AVAILABILITY OF DATA AND MATERIAL
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
CONFLICT OF INTEREST
There is no potential conflict of interest related to this work.
FUNDING STATEMENT
None.
ACKNOWLEDGMENTS
None.