급성 비정맥류 상부위장관 출혈 환자에서 혈관색전술의 임상 효과
Clinical Efficacy of Transcatheter Arterial Embolization for Acute Non-Variceal Gastrointestinal Bleeding
Article information

위장관 출혈은 미국에서 연간 512,925명이 입원하여 입원율과 30일 이내 재입원율이 미국 내 1위를 차지하는 주요 질환 중 하나로 이 중 식도, 위, 십이지장을 포함하는 상부위장관 출혈은 약 40%를 차지한다[1]. 특히, 식도나 위의 정맥류와 같은 만성 간 질환과 관련된 정맥류 출혈과는 별개로 비정맥류 상부위장관 출혈은 인구의 고령화와 이에 따른 항혈전제, 비스테로이드 소염제와 같은 약제 사용의 증가로 인하여 유병률이 꾸준히 지속되고 있다[2]. 양성자펌프억제제의 광범위한 사용 및 내시경 술기의 발달로 대부분의 상부위장관 출혈의 경우 비수술적 방법으로 치료가 가능하게 되었으나, 내시경 지혈술 및 약물 치료에 반응하지 않는 반복적인 재출혈의 경우 혈관색전술이나 수술 등 다른 방법을 고려해야 한다. 이 중 수술적 방법은 대량 수혈이 반복적으로 필요한 경우나 비수술적 치료에 반응하지 않는 쇼크 상태 등에서 일차적으로 고려할 수 있으나 환자의 기저 상태가 불량하여 수술 후 합병증의 발생이 우려되는 경우에는 선택에 신중을 기해야 한다[3].
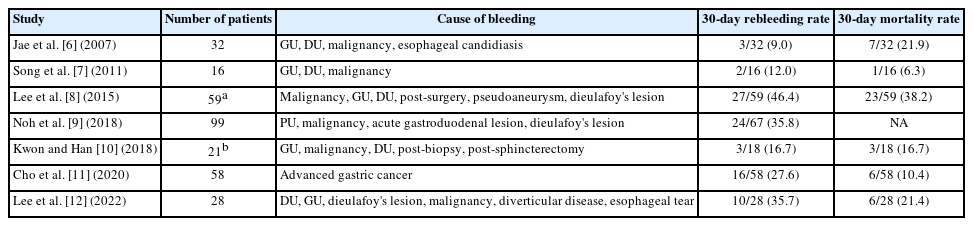
이에 비하여 혈관색전술은 내시경 지혈술에 실패한 경우에 시행 가능한 비수술적 방법으로 수술 전 반복적인 시술이 가능하고 출혈로 인한 사망률은 수술과 비슷하지만 시술 관련 합병증의 빈도가 적은 점 등을 고려하였을 때 비정맥류 상부위장관 출혈 환자의 구제 치료로 우선적으로 고려할 수 있다[4]. 그러나 수술과 혈관색전술을 직접적으로 비교한 연구는 없고 재출혈률은 일반적으로 수술에 비하여 혈관색전술에서 높은 것으로 알려져 있어 현재까지 알려진 임상 데이터를 기반으로 실제 긴급 상황에서 최적의 치료 방침을 결정하기에는 한계가 있다[5]. 국내에서도 과거에 비정맥류 상부위장관 출혈 환자에서 혈관색전술의 임상 경과를 보고한 연구가 다수 발표된 바 있으며, 재출혈률은 9~46%, 시술 후 30일 이내 사망률은 6~38%로 다양하였다[6-12]. 또한, 혈관색전술 후 재출혈에 영향을 미치는 요인으로는 응고장애, 2개 영역 이상에서 색전술을 시행한 경우 등이 있었다[8,12]. 그러나 일부의 연구에서 하부위장관 출혈 환자를 포함하는 등 환자군이 이질적이어서 비정맥류 상부위장관 출혈 환자에서 혈관색전술의 임상적 유용성을 평가하기에는 한계가 있었으며, 모두 단일 기관에서 시행한 연구였기 때문에 전국적인 동향을 알기 어려웠다(Table 1).
Summary of Transcatheter Arterial Embolization for Treatment of Nonvariceal Upper Gastrointestinal Bleeding in Korea
이번에 Kim 등[13]이 시행한 연구는 양성 질환에 의한 급성 비정맥류 상부위장관 출혈로 내시경 지혈술 후 혈관색전술이 필요하였던 환자의 임상상을 평가한 다기관 후향적 연구이다. 국내의 경우 외국에 비하여 상부위장관 내시경 및 시술이 매우 빈번하게 이루어지는 점으로 보아 비정맥류 상부위장관 출혈 치료의 근간은 내시경 지혈술이라고 할 수 있으나, 일부 환자의 경우 내시경 지혈술 후 추가로 혈관조영술 및 혈관색전술이 필요한 경우가 존재한다. 그러나 국내의 혈관색전술의 적응증이나 임상 경과에 대하여 구체적으로 알려진 바는 없으며, 국내 첫 다기관 연구라는 점에서 이 연구가 갖는 의미는 매우 크다고 하겠다. 저자들은 이 연구에서 92명의 환자를 대상으로 임상 데이터를 수집하였고, 대부분의 경우(81명, 88.0%) 소화성 궤양 출혈이었으며 혈관조영술을 시행한 시기는 내시경 지혈술의 실패 후 12시간 이내가 43명(46.7%)으로 가장 많았다. 또한, 77명(83.7%)에서 출혈 병소를 확인 후 특정 동맥을 목표로 하는 선택적 색전술을 시행하였고, 기술적 성공률은 100%, 30일 이내 재출혈은 19명(22.1%), 30일 이내 사망 환자는 6명(5.8%)이었다. 비록 간접 비교이기는 하나 혈관색전술 후 35.5%에서 30일 이내 재출혈률을 보인 외국의 메타분석 연구와 비교하여 임상 성적이 우수하다고 할 수 있다[14]. 또한, 저자들은 다변량 분석을 통하여 응고장애(교차비, 5.66; 95% 신뢰구간, 1.71~18.74)와 선택적 색전술대비 경험적 색전술을 시행한 경우(교차비, 5.71; 95% 신뢰구간, 1.14~28.65)가 혈관색전술 후 30일 이내 재출혈 발생의 위험인자임을 제시하였다. 다만, 비교적 적은 수의 환자를 포함한 후향적 연구이며 양성 비정맥류 상부위장관 출혈 환자만을 대상으로 하였다는 점은 이 연구의 제한점이라고 할 수 있다. 실제로 상부위장관 종양에 의한 출혈의 경우 양성 질환의 출혈에 비하여 일반적으로 재출혈 및 사망률이 높은 점을 감안한다면, 이 연구에서 악성 질환에 의한 출혈을 포함하였을 경우 혈관색전술의 임상 경과는 달라질 가능성이 있다[8].
향후에는 보다 큰 규모의 전국적인 다기관 연구를 통하여 악성 질환을 포함하는 비정맥류 상부위장관 출혈 환자에서 혈관색전술의 임상 경과가 보고되길 기대한다. 나아가서 신속한 혈관색전술의 시행이 필요한 경우에 대한 적절한 지침을 제시할 수 있는 추가 데이터가 발표되기를 기대한다.
Notes
There is no potential conflict of interest related to this work.