Endoscopic Transection for Intramural Esophageal Dissection Caused by a Retropharyngeal Abscess
Article information

Question: A 66-year-old man was admitted with severe pharyngeal pain, dysphagia and dyspnea. Laryngoscopy revealed severe laryngeal edema (Fig. 1A), and neck CT showed a non-collecting retropharyngeal abscess (Fig. 1B). He underwent tracheostomy, and despite antibiotic therapy, his fever and chills persisted with worsening dysphagia. Endoscopy showed diffuse swelling between the upper esophagus and the gastric cardia and an upper esophageal opening discharging pus (Fig. 2A, B). EUS revealed that the swelling of the esophagus and the gastric cardia was caused by submucosal pus accumulation (Fig. 2C), and esophagography showed esophageal dissection between the upper and lower esophagus with a small amount of leakage from the false lumen of the lower esophagus (Fig. 2D).
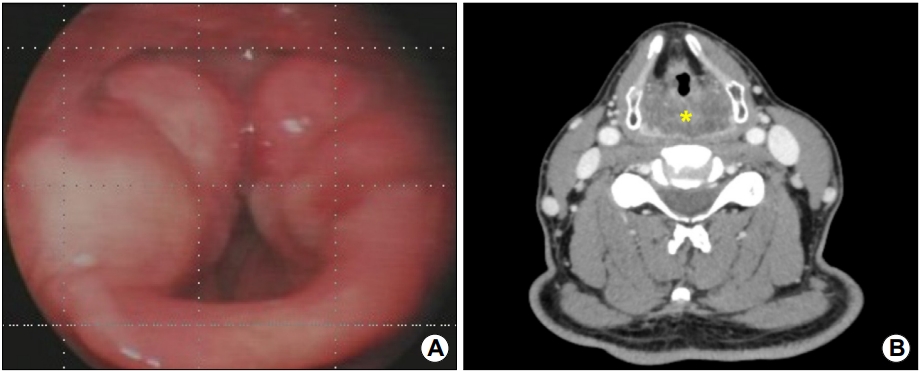
(A) Laryngoscopy shows severe laryngeal edema. (B) Neck CT scan shows a non-collecting retropharyngeal abscess (asterisk).

(A, B) Endoscopy reveals diffuse swelling extending between the upper esophagus and gastric cardia, as well as an upper esophageal opening discharging pus. (C) EUS reveals that the swelling of the esophagus and gastric cardia is caused by hyperechoic floating material in the submucosal layer, suggesting submucosal pus accumulation. (D) Esophagography shows esophageal dissection extending between the upper and lower esophagus, with a small amount of leakage from the false lumen of the lower esophagus (arrow).
What is the appropriate treatment?
Answer: Using a hook-knife (Olympus, Tokyo, Japan), the mucosal bridge between the true and false lumens from the upper to lower esophagus approximately 2 cm proximal to the esophagogastric junction was endoscopically transected; then, endoscopic clipping was performed for a suspected leakage site (Fig. 3A~C and Video 1). Oral intake was resumed, and the patient was discharged 2 weeks later after decannulation. Follow-up endoscopy 2 months later showed a single esophageal lumen (Fig. 3D). The patient was asymptomatic at the 2-year follow-up.
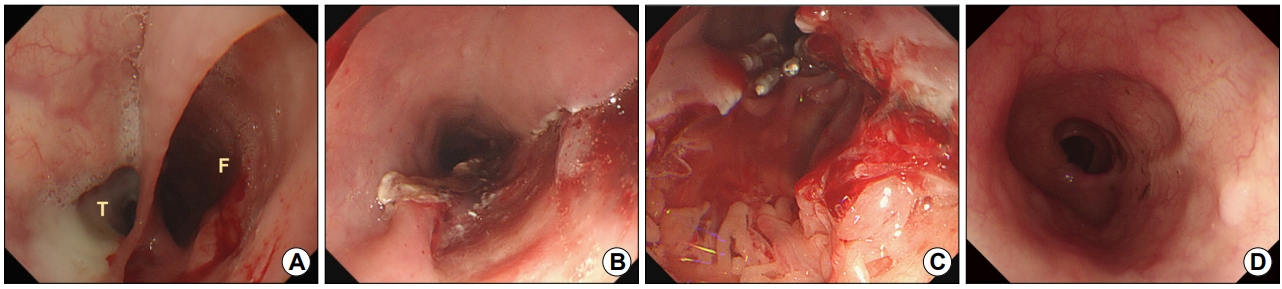
(A, B) Endoscopic transection is performed for the mucosal bridge between the true (T) and false (F) esophageal lumens from the upper to lower esophagus approximately 2 cm proximal to the esophagogastric junction. (C) Endoscopic clipping is performed for a suspected leakage site. (D) Follow-up endoscopy shows a single esophageal lumen.
Intramural esophageal dissection is rare and characterized by sudden severe retrosternal pain, hematemesis, odynophagia, and dysphagia secondary to longitudinal separation of the submucosa from the esophageal muscularis propria.1 It is usually precipitated by a rapid increase in intraesophageal pressure such as intramural hematoma formation.2 Conservative management usually produces favorable outcomes.3 Our patient showed a retropharyngeal abscess that progressed to intramural esophageal dissection and persistent infection and dysphagia despite conservative management; however, he was successfully treated endoscopically.
Notes
No potential conflict of interest relevant to this article was reported.
Supplementary Material
Video 1. Endoscopic transection of the mucosal bridge between the true and false esophageal lumens.(https://doi.org/10.7704/kjhugr.2019.0025.v1)