INTRODUCTION
The gastrointestinal tract is the most common site of extranodal lymphoma involvement. It most often occurs in the stomach, whereas primary esophageal lymphoma is extremely rare, accounting for less than 1% of all primary gastrointestinal lymphomas [1]. Due to its rarity, a standard diagnostic approach and an optimal treatment regimen are yet to be established. In the last decade, there have been only a few case reports on endoscopic submucosal dissection (ESD) as a curative option for primary esophageal mucosa-associated lymphoid tissue lymphoma (PEML) in its early stages [2-5]. This indication has not been validated due to poorly accumulated data. Herein, we present another case of PEML in which a large-sized mass was treated with ESD and a review of previous reports.
CASE REPORT
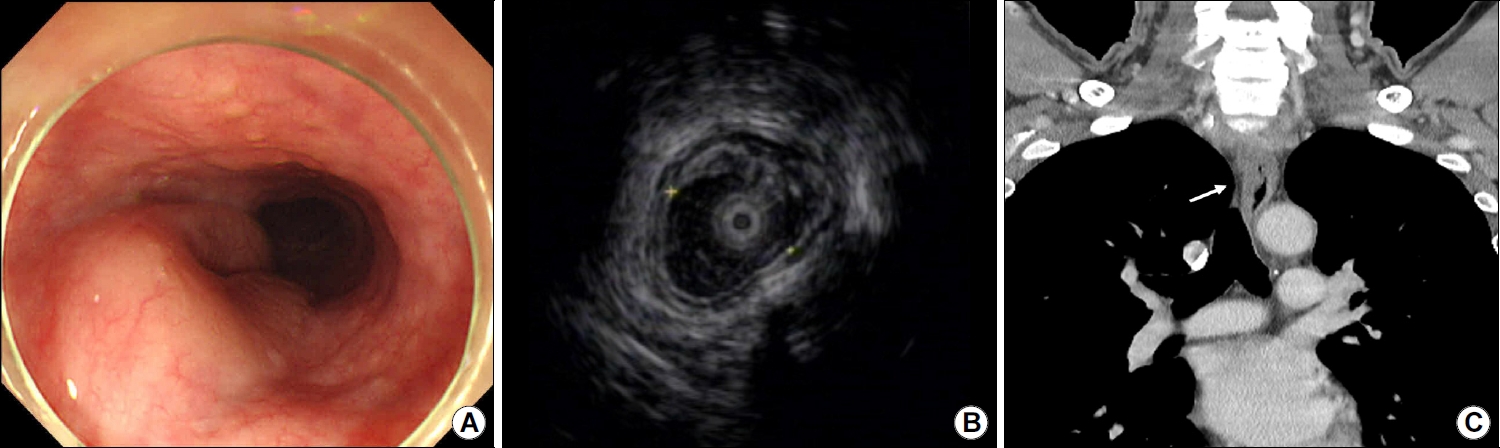
A 54-year-old man was referred to our hospital from a local clinic to evaluate an esophageal subepithelial tumor. The patient complained of pain while swallowing solid food and associated epigastric discomfort that started 6 months prior and gradually worsened. He had hypertension, diabetes mellitus, and a history of bladder cancer and had undergone curative partial cystectomy 2 years earlier. During regular follow-ups, no evidence of cancer recurrence was observed. Physical examination revealed no abnormalities, and the peripheral lymph nodes were not palpable. Laboratory data were within normal ranges, including complete blood count, liver, and kidney function test results, CA 19-9 levels, and CEA levels. Esophagogastroduodenoscopy (EGD; GIF H290, Olympus, Tokyo, Japan) revealed a smooth-surfaced, large-sized, longitudinally extended, horseshoe-shaped subepithelial lesion 23 cm from the incisor (Fig. 1A). Gastroesophageal reflux disease with LA-A (Los Angeles classification) was observed at the esophageal-gastric junction, and there was no abnormality in the stomach, except for atrophic gastritis C-II (Kimura–Takemoto classification). EUS (UM-2R, Olympus) revealed a well-demarcated hypoechoic mass confined to the muscularis mucosal layer (Fig. 1B). Computed tomography (CT) revealed a poorly enhanced, eccentric, and asymmetric wall thickening with intraluminal narrowing of the upper esophagus. No other organs were involved, including the liver, spleen, or lymph nodes (Fig. 1C).
The initial presumptive diagnosis was a benign tumor, such as leiomyoma; however, tumor resection was required to relieve the patient’s dysphagia. Considering the comorbidities associated with esophagectomy, endoscopic resection was selected as the option for coincidental tumor resection and a confirmative diagnosis. Given its well-known advantages in terms of higher en-bloc resection rates and lower recurrence rates than endoscopic mucosal resection (EMR), we performed ESD in the present case.
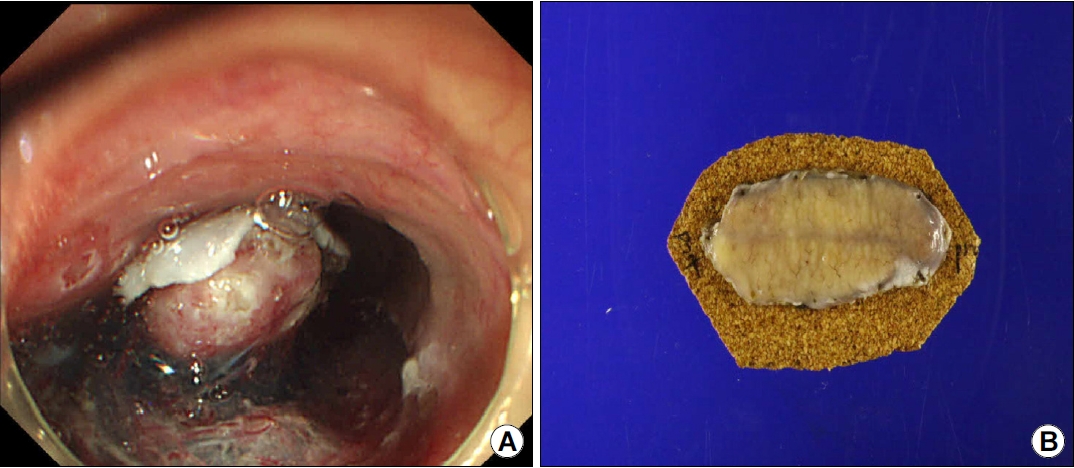
After informed consent was obtained from the patient, ESD was performed under conscious sedation induced by propofol (120 mg) and midazolam (2 mg). The incision site was marked with a J knife, and submucosal injection was performed using a normal saline solution combined with 1:10,000 epinephrine and indigo carmine. After 360-degree precutting with a J knife, the submucosal layer was dissected using a J knife. The tumor was resected without any adverse events (Fig. 2A). The en bloc specimen was 6.1×2.3×0.9 cm in size, and the tumor itself measured across 5.7×2.0 cm (Fig. 2B).
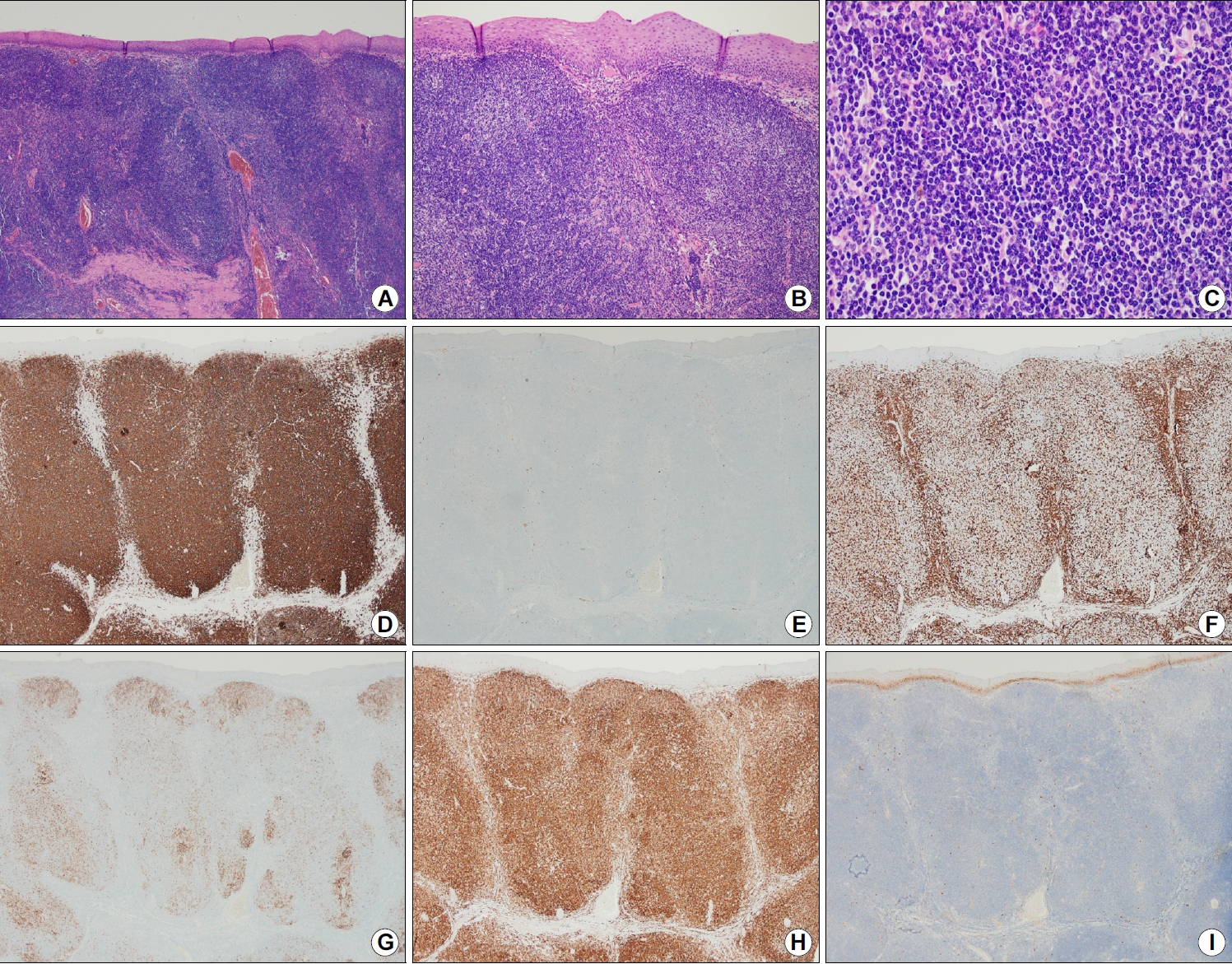
Pathological examination revealed that small lymphocytes with irregular nuclei had heavily infiltrated and expanded the interfollicular zones, leaving small remnant germinal centers. Immunohistochemically, these atypical lymphoid cells stained positive for clusters of differentiation (CD) 20 and BCL-2; however, they were negative for CD5, CD10, CD23, cyclin D1, and BCL-6 (Fig. 3). Because there was no evidence of lymphoma involvement at other sites, the patient was diagnosed with PEML, based on these pathological features. The resected specimen margins were free of lymphoma infiltration. A follow-up endoscopy was performed the following day. Only a clean-based ulcer was present; therefore, the patient started swallowing water. On the second day post-ESD, the patient was tested on a soft diet for tolerability and was discharged. Three months after ESD, the patient’s dysphagia and epigastric discomfort resolved. EGD showed only a scar change at the resection site. The patient was treated with Helicobacter pylori eradication because of an elevated IgG level for H. pylori (13.9 U/mL). The patient has been under regular surveillance for 3 years and has remained recurrence-free.
DISCUSSION
Gastrointestinal lymphoma has two prevalent histological subtypes: diffuse large B-cell lymphoma and mucosa-associated lymphoid tissue (MALT) lymphoma [6]. The latter is a low-grade mature B-cell lymphoma that originates from acquired MALT due to a chronic inflammatory stimulus. Thus, MALT lymphoma can arise at any site ordinarily devoid of lymphoid tissue; however, the esophagus is a very rare site of occurrence [7]. A recent study observed a geographically different prevalence. Unlike in the USA, where diffuse large B-cell lymphoma is the most prevalent, the MALT type is Asia’s most frequent primary esophageal lymphoma [8].
There is no authorized treatment regimen for PEML. The initial treatments for PEML have varied, including surgery, chemotherapy, radiation, H. pylori eradication, EMR, and ESD [3,8]. Generally, MALT lymphomas exhibit indolent characteristic by growing and spreading slowly. Therefore, endoscopic resection or H. pylori eradication could be a less invasive and effective curative treatment option for localized PEML. Table 1 shows that there have been 11 case reports of PEML treated with endoscopic removal and/or H. pylori eradication as a first-line treatment in the English literature. To the best of our knowledge, most of these cases (n=9) were clinically classified as stage I when the Lugano system was used.
Among the 11 cases, the initial treatments for PEML included EMR (n=3), ESD (n=4), and H. pylori eradication (n=4). Similar to our case, PEMLs present as subepithelial tumors in all cases. When visualizing PEML with light endoscopy, it is usually described as a soft subepithelial nodule, fold, or ridge covered by smooth normal mucosa. These tumors tend to extend longitudinally in the craniocaudal direction and are often accompanied by central indentations as they grow; this has already been suggested as a cardinal feature of PEML’s gross appearance [9].
Notably, several methods used for further evaluation in clinical practice are insufficient for detecting PEML. The EUS findings of PEML tends to be nonspecific. PEML usually presents as a well-demarcated subepithelial tumor originating in the muscular mucosa or submucosal layer. In fact, most are hypoechoic; however, they can have focal iso-, hyper-, or variable echogenicity. Leiomyoma, gastrointestinal stromal tumors, and granular cell tumors can also present similar features, requiring differential diagnosis. For these reasons, EUS is more favorable than a differential diagnosis for assessing the depth of invasion and detecting regional lymph node involvement. The CT findings were also non-diagnostic. PEML has generally been reported as a weakly contrast-enhanced mass [9]; however, small masses show only wall thickening and luminal strictures, leading to confusion with esophageal carcinoma.
It is essential but challenging to confirm the diagnosis of PEML due to its subepithelial localization. In 5 (45.5%) of the 11 reported cases, specimens were obtained before the patients were treated. All the 5 cases were diagnosed using standard forceps biopsy. The remaining 6 cases were diagnosed after endoscopic resection.
Since the first reported case in 2014, seven cases of PEML have been treated with EMR [10-12] and ESD [2-5] for which detailed data are available. The masses removed using EMR were all ≤2 cm in size. The masses removed by ESD were measured to be 1.5×0.5 cm, 2.8×1.5 cm, 2×4.3 cm, and unmeasured. They were confined to the deep mucosa or submucosa, and no evidence of metastatic lymph nodes was observed upon CT or EUS examinations. Subsequently, all patients achieved complete resection and were recurrence-free during follow-up. In the present case, we resected a large mass (5.7×2 cm) with ESD, and the patient remains alive to date without recurrence for 3 years. This is the largest-sized mass among the PEML cases presented in Table 1. This indolent malignancy is usually well-demarcated and less invasive; therefore, larger tumors can be resected entirely and more easily than other invasive malignancies if the endoscopist is experienced.
It is well known that H. pylori infection contributes to gastric MALT lymphoma [13,14]. However, unlike gastric MALT lymphoma, the association between PEML and H. pylori infection remains unclear. Four (36.3%) of the 11 reported cases were positive for H. pylori infection. This is lower than the prevalence of 70~80% for H. pylori infection in gastric MALT lymphoma and even lower than the prevalence of 50~70% reported for the general population of East Asia [15,16]. Among the 11 cases, two small (<2 cm) tumors in the distal esophagus treated with solitary H. pylori eradication achieved complete remission within 1 and 3 years of follow-up [17,18]. In contrast, two other patients treated with H. pylori eradication as the first-line therapy showed partial or no responses; however, these were staged as stage II or IV [19,20]. In our case, the patient’s IgG level was elevated due to H. pylori infection; therefore, we performed additional H. pylori eradication as an adjuvant treatment following curative resection.
Although the relationship between PEML and H. pylori remains uncertain, we believe that eradicating H. pylori as an initial or adjuvant treatment can be beneficial. This is because there have been reported cases of PEML in which complete remission was achieved through H. pylori eradication [17,18]. Hence, it is important to not exclude the possibility of an association between PEML and H. pylori. Furthermore, H. pylori eradication is advantageous due to its low cost and its being nearly harmless to the patient. However, it appears to be challenging to achieve complete remission in advanced stages of PEML through H. pylori treatment alone [19,20], suggesting the need for additional treatment alongside H. pylori eradication. The effectiveness of H. pylori eradication in PEML requires further verification.
Since the risk factors for PEML are still unclear, it is speculated that chronic inflammatory stimulation from acid reflux, hot water, chemicals, and other infections could be a potential trigger factor in addition to H. pylori infection [3,4]. However, the previously published cases shown in Table 1 did not report any accompanying esophageal abnormality. In our case, the presence of reflux esophagitis (LA-A, Los Angeles classification) suggests a potential link between chronic inflammatory stimulation and the development of PEML.
In summary, we successfully treated a patient with PEML using ESD and H. pylori eradication therapy, and the patient did not experience recurrence for 3 years after ESD. Therefore, endoscopic resection and adjuvant H. pylori eradication may be preferred for single localized masses. As the clinical profile of PEML is not yet clear, and there is no established treatment, further accumulation of data and additional research are needed for this disease.