ņä£ ļĪĀ
ņ£äņé░ņ¢ĄņĀ£ņĀ£ļź╝ ņןĻĖ░Ļ░ä ļ│ĄņÜ®ĒĢśļŖö ĒÖśņ×ÉļōżņØ┤ ļ¦ÄņĢäņ¦Ćļ®┤ņä£ ļŗżņ¢æĒĢ£ ļČĆņ×æņÜ®ņØ┤ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż[1]. ņ¢æņä▒ņ×ÉĒÄīĒöäņ¢ĄņĀ£ņĀ£(proton pump inhibitor, PPI)ļź╝ ļ│ĄņÜ®ĒĢśļ®┤ ņ£äņĀĆņäĀņØś ļ▓ĮņäĖĒż(parietal cell)ļŖö ņ¢ĄņĀ£ļÉśņ¦Ćļ¦ī ņןĒü¼ļĪ¼ņ╣£ĒÖöņ£Āņé¼(enterochromaffin-like) ņäĖĒż, ņŻ╝ņäĖĒż(chief cell), Ļ░ĆņŖżĒŖĖļ”░(gastrin) ņäĖĒżļŖö ņāüļīĆņĀüņ£╝ļĪ£ ĒÖ£ņä▒ĒÖöļÉśņ¢┤ chromogranin A, Ē׳ņŖżĒāĆļ»╝, ĒÄ®ņŗ£ļģĖĻ▓É(pepsinogen, PG), Ļ░ĆņŖżĒŖĖļ”░ ļČäļ╣äĻ░Ć ņ”ØĻ░ĆĒĢ£ļŗż[2]. ņØ┤ ņżæņŚÉņä£ Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØĆ ņäĀņÖĆņāüĒö╝ ņ”ØņŗØ(foveolar epithelial hyperplasia)Ļ│╝ ļ▓ĮņäĖĒżņØś ļÅīņČ£ņØä ņ£Āļ░£ĒĢśņŚ¼ ņ£äņäĀ ĒśæļČĆ(glandular isthmus)ļź╝ ļ¦ēņĢä ņ£äņĀĆņäĀņØś ļéŁņä▒ ĒÖĢņןņØä ņ£Āļ░£ĒĢ£ļŗż[3]. ĻĘĖļ”¼Ļ│Ā ņØ┤ļ¤¼ĒĢ£ ļ│ĆĒÖöĻ░Ć ņןĻĖ░Ļ░ä ļłäņĀüļÉśļ®┤ ņ£äņĀĆņäĀ ņÜ®ņóģņØ┤ļéś Ļ│╝ĒśĢņä▒ ņÜ®ņóģ, ļŗżļ░£ņä▒ ĒØ░ņāē ņ£ĄĻĖ░ĒśĢ ļ│æļ│Ć(multiple white elevated lesion)ņØ┤ļéś ņĪ░ņĢĮļÅī ļ¬©ņ¢æņØś ņĀÉļ¦ē(cobblestone-like mucosa)ņØ┤ ĒśĢņä▒ļÉ£ļŗż[4].
PPI ļ│ĄņÜ® ĒøäņŚÉ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢśļŖöļŹ░ Ļ▒Ėļ”¼ļŖö ĒÅēĻĘĀ ĻĖ░Ļ░äņØĆ 32.5Ļ░£ņøöļĪ£[5], Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śĻ░Ć 400 pg/mL ņØ┤ņāüņ£╝ļĪ£ ļåÆņ£╝ļ®┤ Ļ│╝ĒśĢņä▒ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢśĻĖ░ ņēĮļŗż[6]. ņ£äņĀĆņäĀ ņÜ®ņóģņØĆ Helicobacter pylori (H. pylori) Ļ░ÉņŚ╝ņØ┤ ņŚåņØäņłśļĪØ ĒśĖļ░£ĒĢśļŖöļŹ░, PPIļź╝ 6Ļ░£ņøö ņØ┤ņāü ļ│ĄņÜ®ĒĢśļ®┤ ļ░£ņāØļźĀņØ┤ 4.71ļ░░ ļåÆņĢäņ¦ĆĻ│Ā 1ļģä ņØ┤ņāü ļ│ĄņÜ®ĒĢśļ®┤ 5.32ļ░░ ļåÆņĢäņ¦äļŗż[7]. PPIļĪ£ ņØĖĒĢ£ ņ£äņĀĆņäĀ ņÜ®ņóģņØĆ ļŗżļźĖ ņ£äņĀĆņäĀ ņÜ®ņóģņŚÉ ļ╣äĒĢ┤ ļéŁņä▒ ĒÖĢņןņØ┤ Ēü¼Ļ│Ā ļ¦Äņ£╝ļ®░, ņäĀņÖĆņāüĒö╝ ņ”ØņŗØĻ│╝ ļ▓ĮņäĖĒż ļÅīņČ£ņØ┤ ņĀĆļ¬ģĒĢśĻ│Ā, Ki-67Ļ│╝ MUC5AC ņŚ╝ņāēņŚÉ ņ¢æņä▒ ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö ņäĖĒżņØś ļ╣äņ£©ņØ┤ ļåÆļŗż[8]. ņĢäņÜĖļ¤¼ ļ▓ĮņäĖĒżņŚÉņä£ ļ░£ĒśäļÉśļŖö aquaporin-4 water channelĻ│╝ KCNQ1 potassium channel ņŚ╝ņāēņŚÉ ņ¢æņä▒ ņåīĻ▓¼ņØä ļ│┤ņØ┤ļŖö Ļ▓ĮņÜ░Ļ░Ć ĒØöĒĢśĻ│Ā, ņÜ®ņóģņŚÉņä£ ņČ£ĒśłņØ┤ Ļ┤Ćņ░░ļÉśĻĖ░ļÅä ĒĢ£ļŗż[9]. ĒĢ£ĒÄĖ, Ļ│ĀļĀ╣ņØś ņŚ¼ņä▒ņŚÉņä£ļŖö ņ£äņĀĆņäĀņØś ļéŁņä▒ ĒÖĢņןĻ│╝ ļ▓ĮņäĖĒż Ļ│╝ĒśĢņä▒ņØ┤ ļŗżļ░£ņä▒ ĒØ░ņāē ņ£ĄĻĖ░ĒśĢ ļ│æļ│Ćņ£╝ļĪ£ Ļ┤Ćņ░░ļÉśĻĖ░ ņē¼ņÜ┤ ļ░śļ®┤[10], Ļ│ĀļĀ╣ņØś ļé©ņä▒ņŚÉņä£ļŖö ņĪ░ņĢĮļÅī ļ¬©ņ¢æņØś ņĀÉļ¦ēņ£╝ļĪ£ Ļ┤Ćņ░░ļÉśĻĖ░ ņēĮļŗż[11]. ņןņāüĒö╝ĒÖöņāØņØ┤ ņ׳ļŖö Ļ│ĀļĀ╣ņØś ļé©ņä▒ņØ╝ņłśļĪØ ņäĀņÖĆņāüĒö╝ ņ”ØņŗØĻ│╝ ļ▓ĮņäĖĒż ļÅīņČ£ņØ┤ ņĀ£ĒĢ£ļÉśņ¢┤ Ēü░ ņÜ®ņóģņØä ļ¦īļōżņ¦Ć ļ¬╗ĒĢśĻ│Ā ņåīĻ▓░ņĀłĒśĢ ņ£ĄĻĖ░ļ¦ī ĒśĢņä▒ĒĢśĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[12].
ņØ┤ ņ”ØļĪĆļŖö H. pylori Ļ░ÉņŚ╝ļĀźņØ┤ ņŚåļŖö 22ņäĖ ļé©ņä▒ņØ┤ 18Ļ░£ņøöĻ░ä PPIļź╝ ļ│ĄņÜ®ĒĢśļŹś ņżæ ĒØæņāēļ│ĆņØ┤ ļ░£ņāØĒĢśņŚ¼ Ļ▓Ćņé¼ĒĢ£ Ļ▓░Ļ│╝, ņ£ä ņ▓┤ļČĆņØś ļ╣äĒøäņÖĆ ņČ£Ēśłņä▒ Ļ│╝ĒśĢņä▒ ņÜ®ņóģņØ┤ ņ¦äļŗ©ļÉ£ ņ”ØļĪĆņØ┤ļŗż. ņÜ®ņóģ ņĀłņĀ£ņłĀĻ│╝ PPI ļ│ĄņÜ®ņØä ņżæļŗ©ĒĢ£ ĒøäņŚÉ ļæÉĻ║╝ņøĀļŹś ņ£äļ▓ĮņØ┤ ĒśĖņĀäļÉśļŖö ĻĄÉĒøłņĀüņØĖ ņ”ØļĪĆļź╝ Ļ▓ĮĒŚśĒ¢łĻĖ░ņŚÉ ļ│┤Ļ│ĀĒĢ£ļŗż.
ņ”Ø ļĪĆ
22ņäĖ ļé©ņ×ÉĻ░Ć 2~3ņŻ╝ Ļ░äĻ▓®ņ£╝ļĪ£ ĒØæņāēļ│ĆĻ│╝ ņ¢┤ņ¦Ćļ¤¼ņøĆņØ┤ ļ░śļ│ĄļÉśņ¢┤ ņÖöļŗż. 1ļģä ļ░ś ļÅÖņĢł ņåŹņō░ļ”╝Ļ│╝ ļ¬ģņ╣ś ĒåĄņ”ØņØ┤ ņ׳ņ¢┤ņä£ 1ļģäĻ░ä omeprazole 40 mgņØä ļ│ĄņÜ®ĒĢśļŗżĻ░Ć ņ”ØņāüņØ┤ ņŗ¼ĒĢ┤ņĀĖņä£ ļ░śļģä ņĀäļČĆĒä░ļŖö pantoprazole 40 mgņ£╝ļĪ£ ļ░öĻ┐öņä£ ļ│ĄņÜ®ĒĢśļŖö ņżæņØ┤ļØ╝Ļ│Ā Ē¢łļŗż. ĒĢśņ¦Ćļ¦ī ņ”ØņāüņØĆ ĒśĖņĀäļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ņłśĻ░£ņøö ņĀäļČĆĒä░ ņŗ¼ĒĢ£ ņ¢┤ņ¦Ćļ¤¼ņøĆņØ┤ 2~3ņŻ╝ Ļ░äĻ▓®ņ£╝ļĪ£ ļ░£ņāØĒ¢łļŗż. ņō░ļ¤¼ņ¦ł ņĀĢļÅäļĪ£ ņ¢┤ņ¦Ćļ¤¼ņÜ┤ ļÆżņŚÉļŖö ļ░śļō£ņŗ£ ļāäņāłĻ░Ć Ļ│ĀņĢĮĒĢ£ ĒØæņāēļ│ĆņØ┤ ļÆżļö░ļźĖļŗżĻ│Ā Ē¢łļŗż. ļ»ĖĻĄŁ ĻĄŁņĀüņØś ļ░▒ņØĖ ļé©ņä▒ņ£╝ļĪ£ ļŗżļźĖ ļ│æļĀźņØĆ ņŚåņŚłņ£╝ļ®░, ĒĢ©Ļ╗ś ļé┤ņøÉĒĢ£ ļ¬©ņ╣£ņØ┤ ņŗżļ”¼ņĢģļ│æ(celiac disease)ņØä ņ¦äļŗ©ļ░øņĢśņ£╝ļéś ņ╣śļŻī ņŚåņØ┤ Ļ┤Ćņ░░ ņżæņØ┤ņŚłļŗż. H. pylori Ļ░ÉņŚ╝ļĀźņØ┤ļéś ņ£äņןĻ┤Ć ņóģņ¢æņØś Ļ░ĆņĪ▒ļĀźņØĆ ņŚåņŚłļŗż. ļé┤ņøÉ ļŗ╣ņŗ£ņØś ĒéżļŖö 176.2 cm, ļ¬Ėļ¼┤Ļ▓īļŖö 79.6 kgņØ┤ņŚłļŗż.
ĒśłņĢĪĻ▓Ćņé¼ņŚÉņä£ ļ░▒ĒśłĻĄ¼ 6.82├Ś103/╬╝m (ņ░ĖĻ│Āņ╣ś 4~10├Ś103/╬╝m), ņĀüĒśłĻĄ¼ 4.66├Ś106/╬╝m (ņ░ĖĻ│Āņ╣ś 4.2~6.3├Ś106/╬╝m), ĒśłņåīĒīÉ 225├Ś103/╬╝m (ņ░ĖĻ│Āņ╣ś 140~400├Ś103/╬╝m), ĒŚżļ¬©ĻĖĆļĪ£ļ╣ł 13.6 g/dL (ņ░ĖĻ│Āņ╣ś 13~16.5 g/dL), Ēśłņāēņåī 38.8% (ņ░ĖĻ│Āņ╣ś 39~49%), mean corpuscular volume 83.4 fL (ņ░ĖĻ│Āņ╣ś 80~98 fL), mean corpuscular hemoglobin (MCH) 29.2 pg (ņ░ĖĻ│Āņ╣ś 27~33 pg), MCH concentration 35.1% (ņ░ĖĻ│Āņ╣ś 32~36%)ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż. Ļ▒┤Ļ░ĢĒĢ£ ļ░▒ņØĖ ļé©ņä▒ņØś ņĀĢņāü Ēśłņāēņåī ņłśņ╣śĻ░Ć 14.0 g/dL ņØ┤ņāüņØ┤ļØ╝ļŖö ņĀÉņØä Ļ░ÉņĢłĒĢĀ ļĢī[13], ĒśłņāēņåīņÖĆ ĒŚżļ¬©ĻĖĆļĪ£ļ╣ł ņłśņ╣śļŖö ļé«ņĢśņ£╝ļéś ļ╣łĒśłļĪ£ ņ¦äļŗ©ļ░øĻ▒░ļéś ņ╣śļŻīļ░øņØĆ ņĀüņØĆ ņŚåļŗżĻ│Ā Ē¢łļŗż. Ēśłņ▓Ł PG I ņłśņ╣śļŖö >160 ng/mL, PG II ņłśņ╣śļŖö >50 ng/mL, Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śļŖö 534.0 pg/mL (ņ░ĖĻ│Āņ╣ś 13~115 pg/mL), chromogranin A ņłśņ╣śļŖö >1,800 ng/mL (ņ░ĖĻ│Āņ╣ś Ōēż108.0 ng/mL)ļĪ£ ļåÆņĢśļŗż. PPI ļ│ĄņÜ® ņØ┤ņÖĖņŚÉ Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØä ņ£Āļ░£ĒĢĀ ļ¦īĒĢ£ ļŗżļźĖ ņøÉņØĖņØ┤ļéś ņ¦łĒÖśņØĆ ņŚåņŚłļŗż.
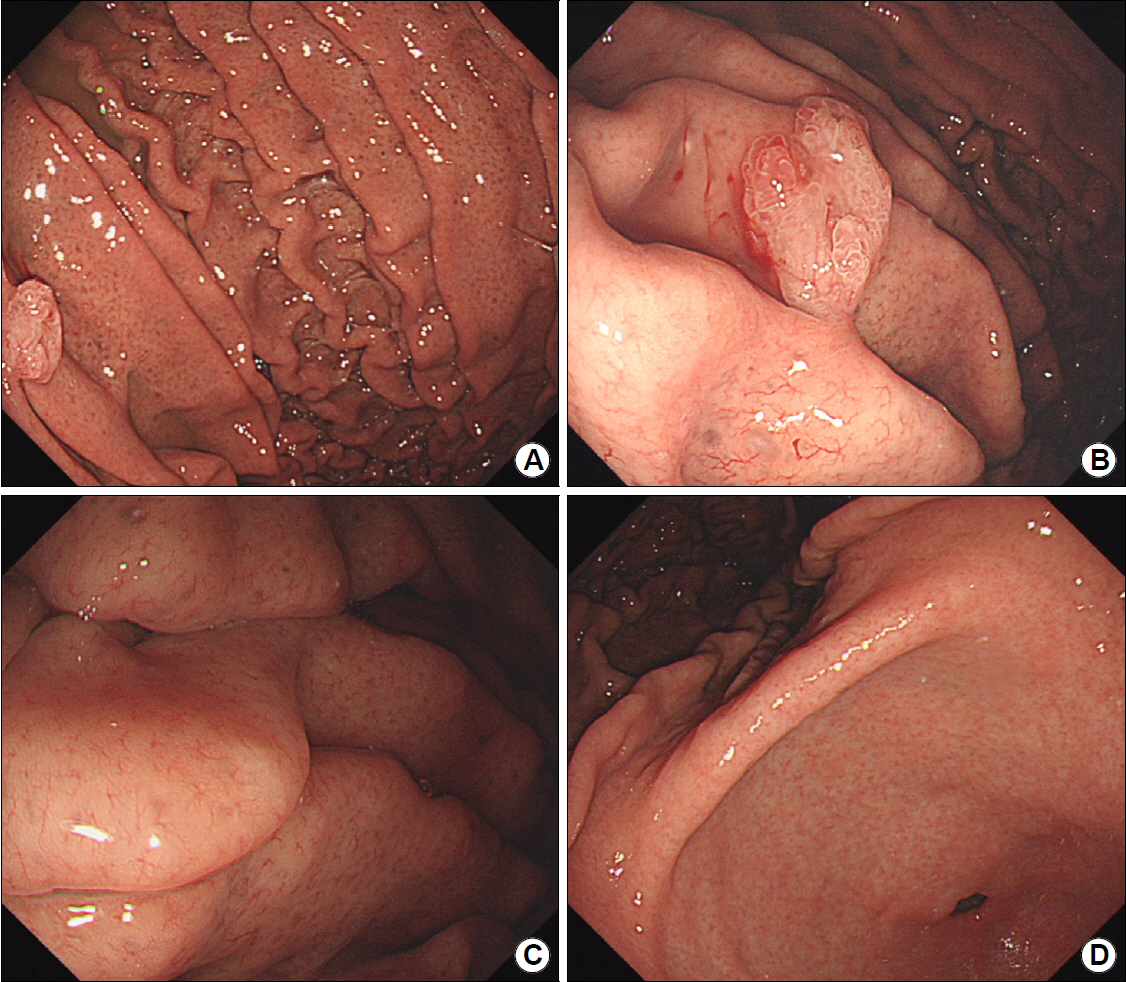
ņ£äļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ņŚÉņä£ ņ▓┤ļČĆņÖĆ ĻĖ░ņĀĆļČĆļŖö ņĀÉļ¦ēņØś ļ╣äĒøäņÖĆ ņ£äņäĀ Ļ░£ĻĄ¼ļČĆ(opening of gastric pit)ņØś ĒÖĢņןņØä ļ│┤ņśĆņ£╝ļéś, ņĀäņĀĢļČĆņÖĆ ņ£äĻ░üņŚÉņä£ļŖö ņØ┤ņāüņØ┤ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż(Fig. 1). ņ£äņŻ╝ļ”ä ņé¼ņØ┤ņŚÉņä£ ļ░£Ļ▓¼ļÉ£ ņÜ®ņóģņŚÉņä£ ņČ£ĒśłņØ┤ Ļ┤Ćņ░░ļÉśņ¢┤ ņÜ®ņóģ ņĀłņĀ£ņłĀņØä ņŗ£Ē¢ēĒ¢łņ£╝ļ®░, Ļ│╝ĒśĢņä▒ ņÜ®ņóģņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 2A, B). ĻĖ░ņĀĆļČĆņÖĆ ņ▓┤ļČĆņŚÉņä£ ņ▒äņĘ©ĒĢ£ ņĪ░ņ¦üņŚÉņä£ļŖö ņ£äņĀĆņäĀņØś ļéŁņä▒ ĒÖĢņןĻ│╝ ņäĀņÖĆņāüĒö╝ ņ”ØņŗØņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░, ļ”╝ĒöäĻĄ¼ņÖĆ ņä¼ņ£ĀņĢäņäĖĒż ņ╣©ņ£żņ£╝ļĪ£ ņØĖĒĢ£ ņĀÉļ¦ē ļ╣äĒøäļź╝ ļ│┤ņśĆļŗż(Fig. 2C, D). H. pylori Ļ░ÉņŚ╝ņØĆ ļ╣äņ╣©ņŖĄņĀüņØĖ Ēśłņ▓Ł ĒĢŁH. pylori immunoglobulin G IgG Ļ▓Ćņé¼ņÖĆ ņ╣©ņŖĄņĀüņØĖ Giemsa ņŚ╝ņāē ļ¬©ļæÉņŚÉņä£ ņ¦äļŗ©ļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░, ņןņāüĒö╝ĒÖöņāØņØ┤ļéś ņ£äņČĢļÅä Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ņ£äĻ░üĻ│╝ ņ▓┤ļČĆņŚÉņä£ ĻĘ£ņ╣ÖņĀüņØĖ ĒśłĻ┤ĆņāüņØ┤ Ļ┤Ćņ░░ļÉśņŚłĻ│Ā, ĒśäĻ░ÉņŚ╝ņØ┤ļéś Ļ│╝Ļ▒░ Ļ░ÉņŚ╝ņØä ņØśņŗ¼ĒĢĀ ļ¦īĒĢ£ ņåīĻ▓¼ņØ┤ ņŚåņ¢┤ņä£ ņÜöņåīĒśĖĻĖ░ Ļ▓Ćņé¼ļŖö ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņĢśļŗż. ĒĢ©Ļ╗ś ņŗ£Ē¢ēĒĢ£ ļīĆņןļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ņŚÉņä£ļŖö ņØ┤ņāüņØ┤ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ņ£äņÜ®ņóģ ņĀłņĀ£ņłĀ ĒøäņŚÉļŖö PPI ļīĆņŗĀ Ē׳ņŖżĒāĆļ»╝ 2 ņ░©ļŗ©ņĀ£(histamine 2 receptor antagonist, H2-blocker)ņØĖ famotidine 20 mgņØä 4ņŻ╝Ļ░ä ĒĢśļŻ© 2ĒÜī ļ│ĄņÜ®ĒĢśļÅäļĪØ ĒĢśņśĆļŗż.
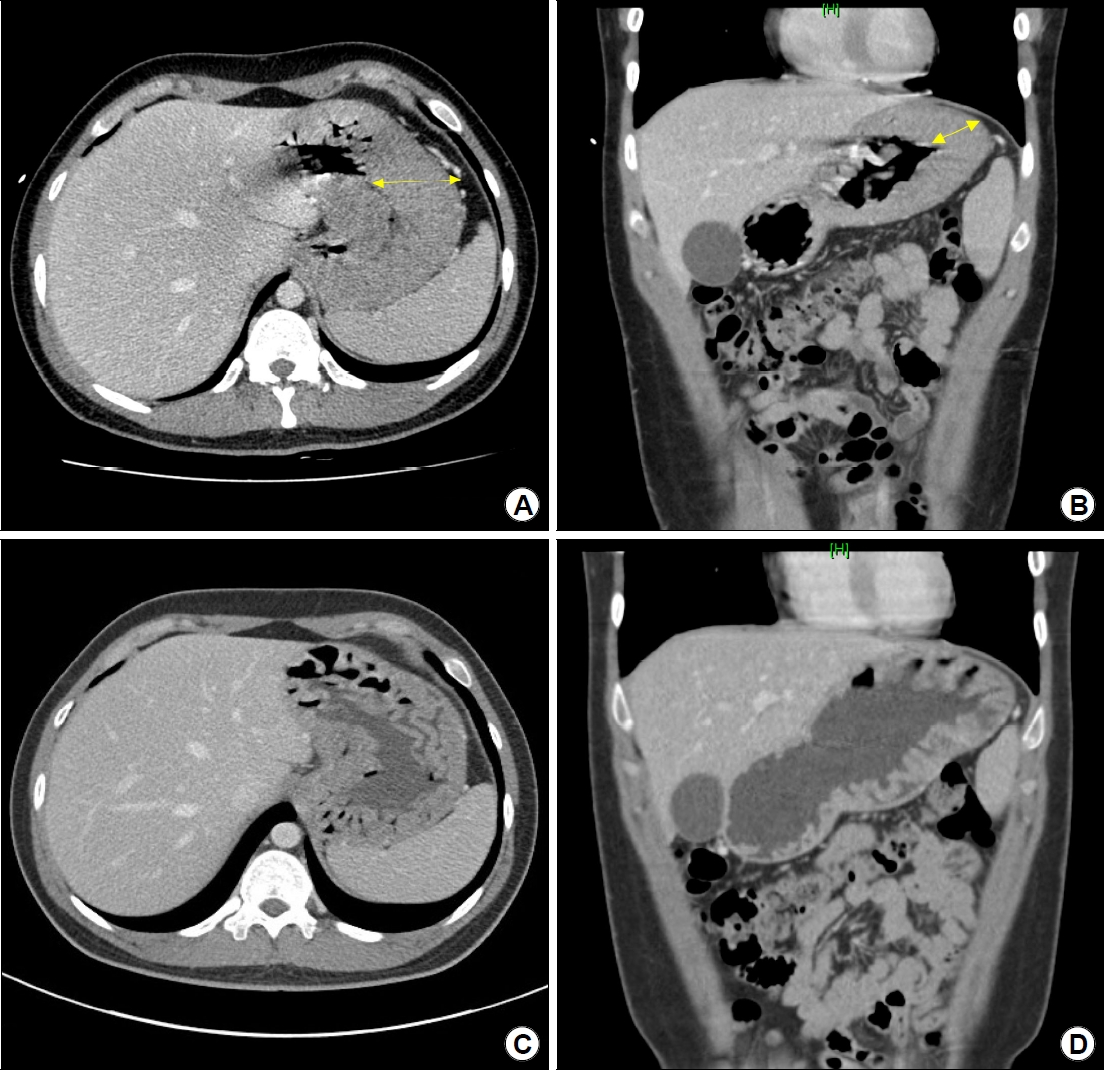
ļ│ĄļČĆ ņ╗┤Ēō©Ēä░ņ┤¼ņśü(CT) Ļ▓Ćņé¼ņŚÉņä£ ņ£äņ▓┤ļČĆņÖĆ ĻĖ░ņĀĆļČĆņØś ņ£äļ▓Į ļ╣äĒøäļź╝ ļ│┤ņśĆļŗż(Fig. 3A, B). ļ│┤ļ¦ī 4ĒśĢņØś ņ¦äĒ¢ēņä▒ ņ£äņĢöņØ┤ļéś ļ”╝ĒöäņóģņØä ņŗ£ņé¼ĒĢśļŖö ļČłĻĘ£ņ╣ÖĒĢ£ ņĪ░ņśüņ”ØĻ░ĢņØ┤ļéś ņŻ╝ļ│Ć ņĪ░ņ¦ü ņ╣©ļ▓ö, ļ”╝ĒöäņĀł ļ╣äļīĆ ļō▒ņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ņ£äļé┤ņŗ£Ļ▓ĮĻ│╝ CT Ļ▓Ćņé¼ ņåīĻ▓¼ņ£╝ļĪ£ ļ│╝ ļĢī, ņ┤łņØīĒīī ļé┤ņŗ£Ļ▓Į Ļ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśļŹöļØ╝ļÅä ņ╣śļŻīĻ│äĒÜŹ(PPI ņżæļŗ©Ļ│╝ ņ£äņÜ®ņóģ ņĀłņĀ£ņłĀ)ņØ┤ ļ░öļĆīņ¦Ć ņĢŖņØä Ļ▓āņ£╝ļĪ£ ņśłņāüļÉśņ¢┤ ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņĢśļŗż. PPIļź╝ ņżæļŗ©ĒĢ£ 3Ļ░£ņøö ĒøäņØś CT ņČöņĀü Ļ▓Ćņé¼ņŚÉņä£ ĻĘ╝ņ£äļČĆņØś ņ£äļ▓Į ļ╣äĒøäļŖö ĒśĖņĀäļÉ£ ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż(Fig. 3C, D). ņČöņĀüĒĢ£ Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śļŖö 517.0 pg/mL, chromogranin A ņłśņ╣śļŖö 950.4 ng/mLļĪ£ Ļ░üĻ░ü Ļ░Éņåī ņżæņØ┤ņŚłļŗż. PPI ļ│ĄņÜ®ņØä ņżæļŗ©ĒĢ£ ņØ┤ĒøäņŚÉ ĒØæņāēļ│ĆņØĆ ņŚåņŚłņ£╝ļ®░, Ēśłņāēņåī ņłśņ╣śļŖö 15.7 g/dL ņØ┤ņāüņ£╝ļĪ£ ņĢłņĀĢņĀüņ£╝ļĪ£ ņ£Āņ¦ĆļÉśņŚłļŗż. ņ”ØņāüņØ┤ ņ×¼ļ░£ĒĢśļ®┤ H2-blockerļź╝ ĻČīĒĢśļĀżĻ│Ā Ē¢łņ£╝ļéś, ņØ┤ņĀäĻ│╝ Ļ░ÖņØĆ ņŗ¼ĒĢ£ ņ”ØņāüņØĆ ņŚåļŗżĻ│Ā ĒĢśņŚ¼ ņ╣śļŻī ņŚåņØ┤ Ļ┤Ćņ░░ ņżæņØ┤ļŗż.
Ļ│Ā ņ░░
ņØ┤ ņ”ØļĪĆļŖö H. pyloriņŚÉ Ļ░ÉņŚ╝ļÉ£ ņĀüņØ┤ ņŚåļŖö ņĀŖņØĆ ļ»ĖĻ░ÉņŚ╝ņ×ÉĻ░Ć PPIļź╝ ņןĻĖ░Ļ░ä ļ│ĄņÜ®ĒĢ£ ĒøäņŚÉ ņäĀņÖĆņāüĒö╝ ņ”ØņŗØĻ│╝ ņ£äņĀĆņäĀņØś ļéŁņä▒ ĒÖĢņןņØ┤ Ļ│╝ļÅäĒĢśĻ▓ī ļ░£ņāØĒĢśņŚ¼ ņāüļČĆņ£äņןĻ┤Ć ņČ£ĒśłĻ╣īņ¦Ć ņ£Āļ░£ĒĢ£ ļō£ļ¼Ė Ļ▓ĮņÜ░ņØ┤ļŗż. ņ¦äļŗ© ļŗ╣ņŗ£ņŚÉļŖö ņ£ä ĻĘ╝ņ£äļČĆņØś ļ╣äĒøäņÖĆ ĒĢ©Ļ╗ś Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░Ļ│╝ chromogranin A ņłśņ╣śņØś ņāüņŖ╣ņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļéś, PPI ļ│ĄņÜ®ņØä 3Ļ░£ņøöĻ░ä ņżæļŗ©ĒĢ£ ĒøäņŚÉ ņ£äļ▓ĮņØś ļ╣äĒøäņÖĆ Ēśłņ▓Ł ņłśņ╣śĻ░Ć ĒśĖņĀäļÉśļŖö ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż.
ņ£äņĀĆņäĀņØś ļ▓ĮņäĖĒżļź╝ ņ¢ĄņĀ£ĒĢśļŖö ņĢĮļ¼╝ ļ│ĄņÜ®ņ£╝ļĪ£ ņØĖĒĢ£ ņ£äņĀÉļ¦ēņØś ļ│ĆĒÖöļŖö ņŻ╝ļĪ£ Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņŚÉ ņØśĒĢ┤ ļ░£ņāØĒĢ£ļŗż(Fig. 4). ņ£äņČĢņØ┤ļéś ņןņāüĒö╝ĒÖöņāØņØ┤ ņŚåļŖö ļ»ĖĻ░ÉņŚ╝ņ×ÉņØ╝ņłśļĪØ Ēü░ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢśĻĖ░ ņē¼ņÜ░ļ®░(Fig. 5), ņ£äņĢöņØĆ ļō£ļ¼╝ļŗż[14]. Ļ│╝ĒśĢņä▒ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢ£ Ļ▓ĮņÜ░ņŚÉļÅä ņśłĒøäļŖö ņ¢æĒśĖĒĢśņŚ¼ PPIļź╝ ņżæļŗ©ĒĢśļŖö Ļ▓āļ¦īņ£╝ļĪ£ļÅä 83%Ļ░Ć ņ×æņĢäņ¦ĆĻ▒░ļéś ņé¼ļØ╝ņ¦äļŗż[15]. ĻĘĖļ¤¼ļéś H. pylori Ļ░ÉņŚ╝ņ×ÉļØ╝ļ®┤ ņäĀņĢöņ£╝ļĪ£ ņ¦äĒ¢ēĒĢĀ ņłś ņ׳ņ£╝ļ»ĆļĪ£, PPI ņżæļŗ©Ļ│╝ ĒĢ©Ļ╗ś ņĀ£ĻĘĀ ņ╣śļŻīļź╝ ĒĢ┤ņĢ╝ ĒĢ£ļŗż[16]. Ē¢źĒøäņŚÉļÅä PPIļéś potassium-competitive acid blocker (P-CAB) ļ│ĄņÜ®ņØä Ēö╝ĒĢ┤ņĢ╝ ĒĢśļŖöļŹ░, P-CABļŖö PPIļ│┤ļŗż ņ£äņé░ ņ¢ĄņĀ£ ĒÜ©Ļ│╝Ļ░Ć ĒāüņøöĒĢ£ ļ¦īĒü╝ Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØś ļ░£ņāØļźĀļÅä ļåÆĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[17]. P-CABļź╝ 1ļģä ņØ┤ņāü ļ│ĄņÜ®ĒĢśļ®┤ 8.8%ņŚÉņä£ ņ£äņĀĆņäĀ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢśĻ│Ā 1.3%ņŚÉņä£ Ļ│╝ĒśĢņä▒ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢ£ļŗżļŖö ļé┤ņÜ®ņØś ņ┤łļĪØņØ┤ 2018ļģä ņØ╝ļ│ĖņåīĒÖöĻĖ░ļé┤ņŗ£Ļ▓ĮĒĢÖĒÜīņŚÉņä£ ļ░£Ēæ£ļÉśņŚłņ£╝ļ®░(unpublished data), 3ļģäĻ░ä vonoprazan 10 mgņØä ļ│ĄņÜ®ĒĢ£ 51ņäĖ ļé©ņä▒ņŚÉņä£ ņäĀņÖĆĒśĢ ņ£äņäĀņĢö(foveolartype gastric adenocarcinoma)ņØ┤ ļ░£ņāØĒ¢łļŗżļŖö ņ”ØļĪĆļ│┤Ļ│ĀļÅä ņ׳ļŗż[18]. ļö░ļØ╝ņä£ ļ│ĄņÜ®ņØ┤ ļČłĻ░ĆĒö╝ĒĢ£ ņāüĒÖ®ņŚÉņä£ļŖö Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØä ņżäņØ┤ĻĖ░ ņ£äĒĢ┤ muscarinic receptor antagonistņØĖ pirenzepineņØä ļ│æņÜ®ĒĢśĻ▒░ļéś[19], H2-blockerņØä ĒĢ©Ļ╗ś Ēł¼ņŚ¼ĒĢ┤ ņÜ®ļ¤ēņØä ņżäņØ┤ļÅäļĪØ ĒĢ£ļŗż[20]. H2-blockerļŖö PPIļéś P-CABņÖĆ ļŗ¼ļ”¼ Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØ┤ļéś PG ņāüņŖ╣ ļ░Å ņ£äņĀĆņäĀ ņ”ØņŗØņØä ņ£Āļ░£ĒĢśņ¦Ć ņĢŖĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[21]. ņĀ£ĻĘĀ ņ╣śļŻī ņŗ£ņŚÉļŖö PPIļź╝ 1~2ņŻ╝ļ¦ī Ēł¼ņŚ¼ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ņĪ░ņ░© ĻĖłĻĖ░ĒĢ┤ņĢ╝ ĒĢ£ļŗżļŖö ņŚ░ĻĄ¼ļŖö ņŚåļŗż. ļŗżļ¦ī ņןĻĖ░Ļ░ä PPIļź╝ Ēł¼ņŚ¼ĒĢ┤ņś© Ļ░ÉņŚ╝ņ×ÉņØś ņ£ä ļé┤ pHļŖö ņØ┤ļ»Ė ņāüņŖ╣ļÉśņ¢┤ ļČłņČ®ļČäĒĢ£ ņ£äņé░ ņ¢ĄņĀ£ļĪ£ ņØĖĒĢ£ ņĀ£ĻĘĀ ņŗżĒī©ņØś Ļ░ĆļŖźņä▒ņØĆ ļé«ņØä Ļ▓āņØ┤ļ»ĆļĪ£ PPI ļīĆņŗĀ H2-blockerļź╝ Ļ│ĀļĀżĒĢ┤ļ│╝ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.
Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØĆ PPIļéś P-CAB ļ│ĄņÜ® ņØ┤ņÖĖņŚÉļÅä ņŗØĒøä, ņŗĀļČĆņĀä, ņ×ÉĻ░Ćļ®┤ņŚŁņä▒ ņ£äņŚ╝, H. pylori Ļ░ÉņŚ╝ņŚÉ ņØśĒĢ£ ņ£äņČĢņä▒ ņ£äņŚ╝, Zollinger-ellison ņ”ØĒøäĻĄ░ņŚÉņä£ļÅä Ļ┤Ćņ░░ļÉśļŖö ņåīĻ▓¼ņ£╝ļĪ£, PPIļź╝ 5ļģäĻ░ä ļ│ĄņÜ®ĒĢśļ®┤ ņĀĢņāü ņłśņ╣śņØś 1.4ļ░░ņØĖ 200 pg/mL ņĀäĒøäļĪ£ ņāüņŖ╣ļÉśĻ│Ā ļ│ĄņÜ® ĻĖ░Ļ░äņØ┤ ĻĖĖņłśļĪØ ņłśņ╣śļÅä ņ”ØĻ░ĆĒĢ£ļŗż[22]. ļ¦īņĢĮ Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śĻ░Ć 1,000 pg/mLļź╝ ņ┤łĻ│╝ĒĢśĻ│Ā ņ£ä ļé┤ pHĻ░Ć 2 ļ»Ėļ¦īņØ┤ļØ╝ļ®┤ Ļ░ĆņŖżĒŖĖļ”░ņóģņØä ņØśņŗ¼ĒĢ┤ņĢ╝ ĒĢ£ļŗż[23]. ļśÉĒĢ£ PPI ņןĻĖ░ ļ│ĄņÜ®ņ×ÉņŚÉņä£ Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śĻ░Ć ļåÆļŗżļ®┤ ņ£ä ņŗĀĻ▓Įļé┤ļČäļ╣ä ņóģņ¢æņØä ņØśņŗ¼ĒĢ┤ņĢ╝ ĒĢ£ļŗż[24]. ņ£Āļ¤ĮņØś ļŗżĻĖ░Ļ┤Ć ņŚ░ĻĄ¼ņŚÉņä£ ļ░£Ēæ£ĒĢ£ ņ£ä ņŗĀĻ▓Įļé┤ļČäļ╣ä ņóģņ¢æ ĒÖśņ×ÉļōżņØś Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śļŖö 964 (585~1,702) pg/mLņśĆņ£╝ļ®░[25], ņØ╝ļ│ĖņØś ļŗżĻĖ░Ļ┤Ć ņŚ░ĻĄ¼ņŚÉņä£ļŖö 2,305 (279~22,956) pg/mLņśĆļŗż[26]. ļö░ļØ╝ņä£ ņØ╝ļ│ĖņŚÉņä£ļŖö PPIļéś P-CAB ņןĻĖ░ ļ│ĄņÜ®ņ×ÉņŚÉņä£ Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śĻ░Ć 700 ng/mL ņØ┤ņāüņ£╝ļĪ£ ļåÆĻ▓ī ļéśņśżļ®┤ ņŗĀĻ▓Įļé┤ļČäļ╣ä ņóģņ¢æņŚÉ ļīĆĒĢ┤ Ļ▓Ćņé¼ĒĢśļŖö ļČäņ£äĻĖ░Ļ░Ć ņĪ░ņä▒ļÉśņ¢┤ ņ׳ņ£╝ļéś, ņ”ØļĪĆĻ░Ć ļō£ļ¼╝ņ¢┤ņä£ ņĢäņ¦ü ņĀäņäĖĻ│äņĀüņ£╝ļĪ£ cutoff valueņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ļŖö ņŚåļŗż. ĒĢ£ĒÄĖ, Ēśłņ▓Ł chromogranin A ņłśņ╣śļŖö 1ĒśĢ ļŗ╣ļć©ļéś ņ×ÉĻ░Ćļ®┤ņŚŁņä▒ ņ¦łĒÖśņŚÉņä£ļÅä ņāüņŖ╣ļÉśļ»ĆļĪ£ Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ņŚÉ ļ╣äĒĢ┤ ņóģņ¢æņŚÉ ļīĆĒĢ£ ņ¦äļŗ©ņĀü Ļ░Ćņ╣śĻ░Ć ļé«ņĢäņä£ ņ╣śļŻī ĒÜ©Ļ│╝ ĒīÉņĀĢņØ┤ļéś ņ×¼ļ░£ ņśłņĖĪņÜ®ņ£╝ļĪ£ļ¦ī ņé¼ņÜ®ĒĢ£ļŗż[27].
ņØ┤ ĒÖśņ×ÉņØś Ļ▓ĮņÜ░, ĒØæņāēļ│ĆņØ┤ ļéśĒāĆļéśĻĖ░ 18Ļ░£ņøö ņĀäļČĆĒä░ PPIļź╝ ļ│ĄņÜ®Ē¢łņ£╝ļ®░(temporal relationship), PPI ņØ┤ņÖĖņŚÉ ļŗżļźĖ ņøÉņØĖņØä ņ░ŠņØä ņłś ņŚåņŚłļŗż(coherence). ļśÉĒĢ£, PPI ļ│ĄņÜ® ĒøäņŚÉ Ļ┤Ćņ░░ļÉ£ Ļ▓Ćņé¼ ņåīĻ▓¼ļōżņØ┤ ĻĖ░ņĪ┤ ļ│┤Ļ│ĀļōżĻ│╝ ņØ╝ņ╣śĒ¢łņ£╝ļ®░(consistency), ĒŖ╣ņØ┤ĒĢ£ ņåīĻ▓¼ļōż(specificity)ņØ┤ņŚłļŗż[1-3,5-8,12]. ļŗżļ¦ī, ņØ┤ ĒÖśņ×ÉĻ░Ć ņČ£ĒśłļĪ£ ņØĖĒĢ£ ņ”ØņāüņØä ļŖÉļéĆ Ļ▓āņØĆ ņ┤Ø 4~5ĒÜīļĪ£ ņłśĒśłņØä ņÜöĒĢĀ ņĀĢļÅäļĪ£ ļ¦ÄņØĆ ņ¢æņØĆ ņĢäļŗłņŚłĻĖ░ņŚÉ ĒŚżļ¬©ĻĖĆļĪ£ļ╣ł ņłśņ╣śļŖö 13.6 g/dL, Ēśłņāēņåī ņłśņ╣śļŖö 38.8%ļĪ£ Ļ▓Įļ»ĖĒĢ£ Ļ░Éņåīļ¦ī ļ│┤ņØĖ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż. ņĢäņÜĖļ¤¼ Ļ│ĀĻ░ĆņŖżĒŖĖļ”░Ēśłņ”ØņØ┤ ņŗ¼ĒĢĀņłśļĪØ ņ£äņĀĆņäĀ ņÜ®ņóģļ│┤ļŗż Ļ│╝ĒśĢņä▒ ņÜ®ņóģņØ┤ ļ░£ņāØĒĢśĻĖ░ ņē¼ņÜ┤ļŹ░[28], ņØ┤ ĒÖśņ×ÉņŚÉņä£ļÅä Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░ ņłśņ╣śĻ░Ć ļåÆĻ▓ī ņĖĪņĀĢļÉśņ¢┤ Ļ│╝ĒśĢņä▒ ņÜ®ņóģĻ│╝ņØś ņŚ░Ļ┤Ćņä▒ņØä ņ░ŠņØä ņłś ņ׳ņŚłļŗż(strength). ļéśņĢäĻ░Ćņä£ PPIļź╝ ņżæļŗ©ĒĢ£ ņØ┤ĒøäņŚÉ ņ£äļ▓ĮņØś ļ╣äĒøäĻ░Ć 3Ļ░£ņøö ļ¦īņŚÉ ĒśĖņĀäļÉśņŚłĻ│Ā, Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░Ļ│╝ chromogranin A ņłśņ╣śļÅä Ļ░ÉņåīĒĢśļŖö ņŚ░Ļ┤Ćņä▒ļÅä Ļ┤Ćņ░░ļÉśņŚłļŗż. ņØ┤ ņ”ØļĪĆņŚÉņä£ chromogranin A ņłśņ╣śĻ░Ć ņĄ£Ļ│Āņ╣śņØĖ >1,800 ng/mLņŚÉņä£ 950.4 ng/mLļĪ£ ļ╣Āļź┤Ļ▓ī Ļ░ÉņåīĒĢśļ®┤ņä£ ņ”ØņāüļÅä ĒśĖņĀäļÉ£ Ļ▓āņ£╝ļĪ£ ļ│╝ ļĢī, ĒÖśņ×ÉĻ░Ć ņ▓śņØīņŚÉļŖö ņ£äņé░Ļ│╝ļŗżļĪ£ ņØĖĒĢ┤ PPIļź╝ ļ│ĄņÜ®ĒĢśĻĖ░ ņŗ£ņ×æĒ¢łņ¦Ćļ¦ī ņØ┤ĒøäņŚÉļŖö PPI ļČĆņ×æņÜ®ņ£╝ļĪ£ ņØĖĒĢ┤ ņ£ä ĻĘ╝ņ£äļČĆĻ░Ć ĒīĮņ░ĮĒĢśļ®┤ņä£ ņ”ØņāüņØ┤ ļ░£ņāØĒĢ£ Ļ▓āņ£╝ļĪ£ ņČöņĀĢļÉ£ļŗż. ņ£ä 5Ļ░Ćņ¦Ć ĒŖ╣ņä▒ļōż(temporal relationship, coherence, consistency, specificity, strength)ņØä ņóģĒĢ®ĒĢĀ ļĢī, ņØ┤ ņ”ØļĪĆļŖö ņןĻĖ░Ļ░ä PPI ļ│ĄņÜ®ņ£╝ļĪ£ ņØĖĒĢ£ ņĢĮņĀ£ņä▒ ļ│æļ│Ćņ£╝ļĪ£ ĒĢ┤ņäØļÉ£ļŗż.
Ļ▓░ļĪĀņĀüņ£╝ļĪ£ ņØ┤ ņ”ØļĪĆļŖö ņĀŖņØĆ ļéśņØ┤ņØś ļ»ĖĻ░ÉņŚ╝ņ×ÉĻ░Ć 18Ļ░£ņøöĻ░ä PPIļź╝ ļ│ĄņÜ®ĒĢśļ®┤ņä£ ĻĖ░ņĀĆļČĆņÖĆ ņ▓┤ļČĆņØś ņ£äņĀÉļ¦ēņØ┤ Ļ│╝ļÅäĒĢśĻ▓ī ņ”ØņŗØĒ¢łĻ│Ā, ļÅÖļ░śļÉ£ Ļ│╝ĒśĢņä▒ ņÜ®ņóģņØ┤ ņČ£ĒśłļÉ£ Ļ▓ĮņÜ░ņØ┤ļŗż. ņČ£Ēśłņä▒ ņÜ®ņóģņŚÉ ļīĆĒĢ£ ļé┤ņŗ£Ļ▓Į ņĀłņĀ£ņłĀĻ│╝ PPIļ│ĄņÜ® ņżæļŗ© ņØ┤ĒøäņŚÉ ĒØæņāēļ│ĆņØĆ ņé¼ļØ╝ņĪīņ£╝ļ®░, CTņŚÉņä£ļŖö ņ£äļ▓ĮņØś ļČĆņóģņØ┤ ĒśĖņĀäļÉśņŚłĻ│Ā Ēśłņ▓Ł Ļ░ĆņŖżĒŖĖļ”░Ļ│╝ chromogranin Aņłśņ╣śļŖö Ļ░ÉņåīĒ¢łļŗż. ņ£äņČĢņØ┤ļéś ņןņāüĒö╝ĒÖöņāØņØ┤ ņŚåļŖö ļ»ĖĻ░ÉņŚ╝ņ×ÉĻ░Ć ņןĻĖ░Ļ░ä PPIļź╝ ļ│ĄņÜ®ĒĢ£ ņØ┤ĒøäņŚÉ ņ£äņןĻ┤Ć ņČ£ĒśłņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ļŗżļŖö Ļ▓āņØä ņāüĻĖ░ņŗ£ņ╝£ņżĆ ņ”ØļĪĆņśĆļŗż. Ļ░łņłśļĪØ ĻĄŁļé┤ņŚÉņä£ļÅä ļ»ĖĻ░ÉņŚ╝ņ×ÉņØś ļ╣äņ£©ņØ┤ ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳Ļ│Ā, PPIļéś P-CABļź╝ ņןĻĖ░ ļ│ĄņÜ®ĒĢśļŖö ņé¼ļ×īļōżļÅä ņ”ØĻ░ĆĒĢśĻ│Ā ņ׳ņ£╝ļ»ĆļĪ£ ĒŖ╣ņ¦ĢņĀüņØĖ Ļ▓Ćņé¼ ņåīĻ▓¼ļōżņØä ņóģĒĢ®ĒĢ┤ņä£ ļ│┤Ļ│ĀĒĢśņśĆļŗż.