서 론
헬리코박터 파일로리는 위축성 위염과 장상피화생, 소화성 궤양, 점막관련림프조직 림프종의 원인이 되며, 궁극적으로 위암을 초래할 수 있다는 것은 잘 알려져 있다. 여러 가지 연구를 통하여 헬리코박터 파일로리가 위암의 원인이라는 것이 증명되었기에 2013년부터 일본에서는 전 국민을 대상으로 국가 주도의 제균 치료를 시행하고 있다. 헬리코박터 파일로리에 대한 제균 치료가 빈번해지고 약제 노출이 많아지면서 일부 항생제에 대한 내성률이 증가하고 있다. 또한 지역에 따라 항생제 내성의 양상이 달라 해당 지역별로 개별화한 제균 요법의 개발이 점차 중요하게 되었으며, 새로운 처방의 조합이나 신약 개발의 요구가 증가되고 있다. 본고에서는 최근 헬리코박터 파일로리 제균의 변화된 동향과 새롭게 추가된 방법에 대하여 기술하기로 한다.
본 론
1. 기존 제균 치료 조합
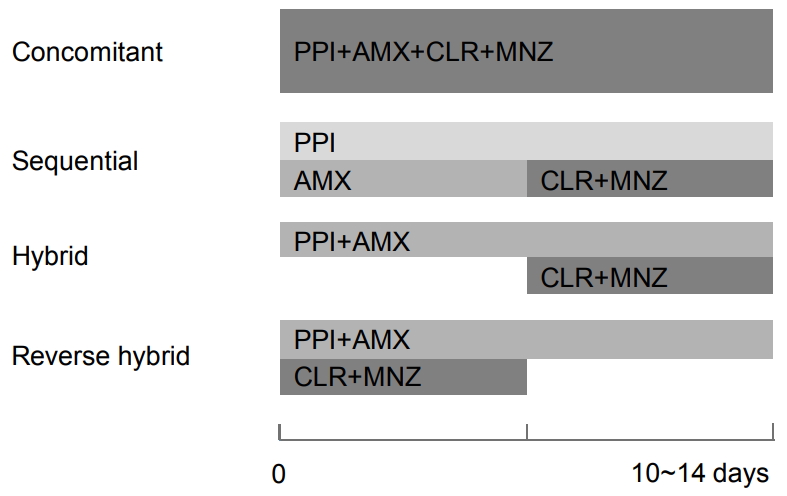
지금까지 사용하고 있는 제균 요법은 몇 가지로 거의 통일되어 있으며 다음과 같다[1]. 가장 대표적인 치료의 조합은 표준삼제요법(standard triple therapy, STT)으로, 전 세계적으로 가장 기본적인 1차 치료법이고 최근까지 국내에서도 가장 널리 사용되고 있다. 양성자펌프억제제(proton pump inhibitor [PPI], standard dose b.i.d.)에 amoxicillin (AMX, 1 g b.i.d.), clarithromycin (CLR, 500 mg b.i.d.)을 추가하여 7~14일 투여하는 조합이나 점차 CLR 내성의 증가로 제균 실패율이 높아지고 있다. Bismuth (BMT) 포함 사제요법은 PPI+BMT+tetracycline (TTC, 500 mg qid)+metronidazole (MNZ, 500 mg tid)의 조합을 7~14일 투여하는 방법으로 전통적으로 국내외 가이드라인에서 2차 치료법으로 인정하는 치료법이다. 순차요법(sequential therapy)은 총 10일간의 투약 중 첫 5일을 PPI+AMX 투약 후 다음 5일간 PPI+CLR+MNZ을 투여하는 법이다. BMT 불포함 사제요법은 동시요법(concomitant therapy)이라고도 하며 PPI+CLR+AMX+MNZ로 10~14일 투약하는 방법이다. 혼합요법(hybrid therapy)은 첫 7일간 PPI+AMX를 투여하고 후반 7일간 PPI+AMX+CLR+MNZ을 투여하는 방법이다. 역혼합요법(reverse hybrid therapy)은 CLR+MNZ의 투여 시점을 전반 7일로 옮긴 방법이다(Fig. 1). 난치성 상황에서 구제 요법으로는 levofloxacin (LFX, 500 mg b.i.d.) 기반 삼제요법으로 PPI+AMX+LFX를 10일간 투여하거나 rifabutine (RFB, 150 mg b.i.d.) 기반 삼제요법으로 PPI+AMX+RFB를 10~14일 투여한다. 각각의 특성을 열거하면 다음과 같다[1,2]. STT의 가장 큰 단점이 CLR 내성 증가에 따른 제균율 감소인데, 국내 가이드라인에서도 CLR 내성이 15~20%를 넘을 경우 1차 치료로 STT 대신 BMT 기반 사제요법을 권고하고 있다[3]. BMT 기반 사제요법은 MNZ 내성에 가장 큰 영향을 받는데 현재까지 제균율 감소세는 뚜렷하지 않고 치료 기간을 1주로 할지 2주가 더 좋을지에 대해서는 아직 논란이 있는 상황이다. 순차요법은 STT의 제균율 감소에 대응하기 위하여 2000년 이탈리아에서 개발된 방법으로, 전반부에 AMX+PPI 투여로 균주의 수가 줄고 병독성이 낮은 알균 유사형(coccoid form)으로 바뀌면 후반부의 macrolide+imidazole+PPI 삼제요법 치료 효과가 극대화된다는 것이다[4-6]. 이후로 점차 부정적인 평가가 많아졌는데, 전·후반에 투여되는 약제가 상이하여 순응도 저하가 우려되고, CLR과 MNZ을 동시에 사용하므로 제균에 실패한 경우 2차 치료 약제 선택에 어려움이 예상되기 때문이다[3]. 그리고 순차요법의 높았던 제균율이 순차적인 약물 투여 때문인지 아니면 삼제요법에 포함되지 않은 MNZ 추가 때문인지 불명확하다는 비판에 따라 동시요법이 제안되었다[7]. 제균율을 평가할 때 intention-to-treat (ITT) 방식과 per-protocol (PP) 방식으로 나누어서 비교하는데, 그간 국내에는 동시요법이나 순차요법이 STT에 비하여 유의한 차이가 없다고 알려졌으나 최근 보고된 국내 다기관 무작위 대조군 연구에서 1차 치료로 기존 STT 1주 치료보다는 10일 동시요법(동시요법 81% vs. STT 64% by ITT; 동시요법 91% vs. STT 71% by PP)과 10일 순차요법(순차요법 76% vs. STT 64% by ITT; 순차요법 85% vs. STT 71% by PP)이 더 효과적이었고, 3가지 치료군에서 순응도나 심각한 부작용의 차이는 없었다[8].
2. 항생제 감수성 검사에 기반한 치료
최근까지 중국을 중심으로 헬리코박터 파일로리 제균의 주력 항생제인 CLR, MNZ, LFX의 항생제 내성률이 심각하게 상승하였고, 국내의 내성률 상승도 두드러져 CLR 10~20%, MNZ 31~50%, LFX 21~30% 범주에 들어가는 것으로 파악되었으며, MNZ과 LFX은 일본보다도 높은 내성률을 보였다[9].급격히 상승하는 항생제 내성률에 대하여 해당 균주에 대한 항생제 내성 검사를 시행하여 적극적으로 적절한 항생제를 선택한 후 치료법을 결정하는 것이 가장 적극적인 대처법이며, 특히 1, 2차 치료에 실패한 경우라면 3차 치료의 성공을 보장하기 위하여 항생제 감수성 검사에 기반한 치료가 가장 바람직한 방법이다. 항생제 내성률이 높은 지역에서 2회 이상 제균에 실패한 후 항생제 감수성 검사를 시행하는 것보다 1차 치료 전 감수성 검사를 하는 것이 이점이 더 크다고 알려졌다[2].
한 국내 연구에서는 1차 치료에서 배양검사를 토대로 제균약제를 선정한 경우가 10일간의 경험적 순차요법보다 제균율이 높았다[10]. 여러 차례 제균에 실패한 경우도 배양을 통한 항생제 감수성 검사 후 제균을 시도하여 60%의 성공을 거두었다[11]. 헬리코박터 파일로리는 배양이 까다로운데, 비교적 숙련된 인력을 보유한 센터 내에서도 배양 성공률이 72%였고, 이를 토대로한 제균 성공률도 44%에 그쳤다[12]. 더욱이 자체 배양 여건이 없는 대부분의 병원은 검체 이송과 조직 처리 과정의 오류로 추가적인 배양 성공률 저하가 예상된다. 헬리코박터 파일로리를 직접 배양하는 것이 어려워 항생제 내성에 대한 분자생물학적 검사들이 개발되었다. 헬리코박터 파일로리 유전자의 점돌연변이는 항생제 내성과 관련이 있는데, macrolide, MNZ, quinolones, rifampins, AMX, TTC의 내성과 관련된 유전자는 각각 23S rRNA, rdxA & frxA, gyrA, rpoB, plp1, 16S rRNA라고 알려져 있다[13]. 이를 분자생물학적 기법으로 검사하면 해당 항생제의 내성 상황을 가늠할 수 있다. 따라서 23S rRNA의 점돌연변이 여부로 CLR 내성을 예측할 수 있고 이를 위 조직의 실시간 역전사 중합효소연쇄반응 기반으로 검사를 하였을 때 표현형과의 일치율이 95%에 달하였다[14]. CLR과 더불어 내성이 많은 LFX의 내성은 gyrA의 점돌연변이와 관련이 있었다[15]. 최근에는 포르말린 처리 후 파라핀 매몰된 조직의 헬리코박터 파일로리 DNA에 대한 차세대 염기서열 분석으로 23S rRNA, gyrA, 16S rRNA 유전자의 돌연변이를 검출하는 기법이 미국 오하이오 코호트를 대상으로 연구되었는데, 23S rRNA에서 빈번한 점돌연변이 위치는 A2142G 또는 A2413G였고, 제균 실패군의 88%와 제균 성공군의 10%에서 이곳에 점돌연변이가 발견되었다(P<0.001) [16]. gyrA 유전자에서는 N87T 또는 N87I, 16S rRNA 유전자에서는 A928C, A926G가 빈번한 돌연변이 위치였다. 제균 효과와의 비교에서 한 가지 유전자 돌연변이가 있을 때의 제균 실패율은 18.5%인데 두 가지 이상의 유전자 돌연변이가 있을 때의 제균 실패는 69%에 달하여 돌연변이 유전자가 많을수록 치료 실패가 많았다[16]. 국내 연구에서도 23S rRNA의 점돌연변이에 대한 중합효소연쇄반응에 소요되는 비용이 환자당 4달러 이하로 경험적 치료보다 가격-효과 면에서 이점이 있었다[17].
4. 비BMT 기반 치료
최근 대규모 메타분석에서 5~10일 동시요법은 5~10일 STT에 비하여 우월하였으나 14일 STT보다는 우월하지 않았다[24]. 스페인에서 있었던 전향적 단면 분석 연구에서는 동시요법의 제균율은 98%로 BMT 기반 사제요법의 제균율(94%)과 유사하였다[25]. 순차요법은 CLR과 MNZ에 감수성이 있는 균주에서 10일 순차요법의 제균율이 97%, MNZ 내성 균주에서는 96%, CLR 내성 균주에서는 93% 그리고 CLR과 MNZ 동시 내성 균주에서도 83%의 제균율을 보여주었다[26]. 혼합요법은 동시요법과 순차요법의 장점을 모아 치료하는 방식으로 개발되었으나 합병증이 많고 복약 순응도가 떨어진다는 단점이 있었고, 이후 연구에서 2주간의 순차요법과 혼합요법의 차이가 없다고 알려졌다. 혼합요법의 단점을 보완하고 간소화하기 위하여 역혼합요법이 개발되었는데, 대만에서 시행한 역혼합요법은 14일 BMT 기반 사제요법과 동일한 효과를 보여주었다[27]. 한 메타분석 연구에서는 CLR 내성이 낮은(<15%) 지역에서는 혼합요법이 가장 효과적이고, 내성이 높은(>15%) 지역에서는 순차요법의 제균율이 높았다고 보고하였다[28].
5. BMT 기반 치료
BMT는 부작용이 문제가 될 수 있으나 제균 치료에 긍정적인 효과가 있다. 헬리코박터 파일로리의 부착을 저해하고 효소와 ATP 생성을 억제하는 등 기존 항생제와는 다른 방법으로 제균 효과를 나타내며, 아직 내성 보고가 없고 항생제 병용 시 상승 작용이 있어 MNZ이나 CLR 내성 헬리코박터 파일로리의 항생제 감수성을 증가시키는 효과가 있다[29].
BMT의 상승 작용에 대한 연구로, 1차 치료에서 BMT를 추가하였을 때의 제균율은 유럽과 중국에서 공히 88%였다[30,31]. BMT 기반 사제요법의 문제는 복약 방법이 대단히 까다롭다는 것이다. 최근 BMT와 2개의 항생제를 합쳐 단일제형(three-in-one) 캡슐을 이용한 연구가 중국과 이탈리아에서 있었는데, 중국에서 보고한 제균율은 86~87%였고[32], STT의 PPI 용량을 줄이고 BMT를 추가한 경우에도 제균율의 차이가 없었다[33]. 페니실린 알레르기가 있는 환자를 대상으로 PPI+CLR+MNZ 삼제요법군보다 BMT를 추가한 군에서 제균율이 유의하게 상승하였고(ITT 64% vs. 85%; PP 70% vs. 96%), BMT 추가 시 CLR 내성군과 MNZ 내성군의 제균율을 모두 향상시켰다[34].
이탈리아에서 단일제형 캡슐을 이용한 BMT 사제요법의 제균율(ITT)은 1차 치료 91%, 2차 치료 88%, 3차 치료 92%였고, 부작용은 32%였으며 6%만 중도 탈락하였다[35]. 이와 유사한 연구가 스페인에서도 있었는데 제균율이 1차 치료 78%, 2차 치료 85%, 3차 치료 61%였다[36].
10일간의 단일제형 캡슐을 이용한 BMT 사제요법에 대한 메타분석에서 PPI 용량, CLR이나 MNZ 내성, 과거 CLR 사용 여부에 관계없이 1차와 2차 제균율이 모두 90%에 달하였다[37]. 국내 메타분석에서는 1차 치료에 BMT를 포함한 경우 제균율(PP)이 86%였고 BMT를 포함하지 않았을 때와의 전체적인 교차비(OR)가 1.83이었으며 무작위 대조군 연구만 모았을 때는 2.81이었다[38]. CLR 기반 14일 BMT 사제요법에서 CLR을 절반만 사용하였을 때도 제균율이 차이가 나지 않았고[39], 국내의 한 연구에서는 2차 치료로 moxifloxacin 기반의 14일 치료보다 7일간의 BMT 기반 치료의 제균율이 더 높았다(74% vs. 94%) [40]. BMT 기반 사제요법에서 LFX 500 mg q.d.와 200 mg b.i.d.는 제균율의 차이를 보이지 않았다[41].
6. 이제요법
CLR과 LFX에 대한 내성이 꾸준히 증가하고 있으나 AMX과 TTC에 대한 1차 내성은 전 지역에 걸쳐 낮게 유지되고 있다[2]. PPI와 AMX 이제요법은 20년 전까지는 사용되었으나 CLR 도입 후 빠르게 삼제요법으로 대체되었다가 CLR 내성이 증가하면서 이제요법에 대한 재조명이 시작되었다. 고용량의 기준은 AMX을 하루 2 g 이상 투여하여 최저 약물 농도를 높이는 것으로 보통 1 g tid 또는 750 mg qid 형태로 투여하며, 중국과 대만 등의 보고에서는 BMT 기반 사제요법이나 동시 치료의 제균율에 필적하는 성적을 보여주었다[42-44]. 고용량 AMX은 다른 치료 조합에도 적용될 수 있는데, 고전적인 BMT 기반 사제요법에서 TTC 대신에 고용량 AMX (3 g/day)을 사용한 결과 제균율이 유의하게 높았고 부작용도 적었다[45]. 또 RFB 삼제요법에서 고용량 AMX을 사용하고 RFB을 절반 용량으로 낮추어도 높은 제균율을 보였다[46].
7. 기타 항생제
항생제 내성이 늘어나고 있어 이에 대한 대책이 필요하며 아직 AMX, TTC, RFB, sitafloxacin에 대한 내성은 드물기 때문에 항생제 내성이 문제가 되는 지역에서는 이런 약제의 조합을 사용해볼 수 있다. RFB은 백혈구 감소증 우려가 있는 약제이나 이탈리아에서 1회 이상의 제균 실패의 경험이 있고 CLR, MNZ, LFX에 3중 내성이 있는 균주를 가진 환자를 대상으로 AMX 1 g tid, esomeprazole 40 mg b.i.d., RFB 150 mg q.d. (half dose)로 12일 치료를 시행한 결과 높은 제균율을 보여주었고(ITT 83%, PP 89%) [46], 1, 2차 제균에 실패하였던 사람들을 대상으로 14일간의 RFB 기반 치료를 한 결과 제균율이 71%였다[47]. SFX도 항생제 내성이 매우 적은 약제로, 일본에서는 3차 구제 요법에 사용하고 있다[48].
8. 칼륨 경쟁적 산분비 억제제
PPI보다 위산 분비 억제능이 뛰어나다고 알려진 vonoprazan (VPZ)이 일본에서 개발된 이후 이 약제를 위시한 칼륨 경쟁적 산분비 억제제(potassium-competitive acid blocker)의 제균 치료에서의 역할이 관심을 모으고 있다. 한 메타분석에서 CLR 내성 균주에 대하여 VPZ 기반 삼제요법은 PPI 기반 삼제요법에 비하여 우월하였고(82% vs. 40%, P<0.0001), CLR 감수성 균주에 대해서는 유사하였다[52]. 경험적 치료로 VPZ 기반 삼제요법의 제균율은 PPI 기반 삼제요법보다 우월한 성적을 보여주었다(ITT 93% vs. 79%, P<0.001; PP 95% vs. 86%, P<0.001)[53]. 후향적 연구로 CLR 기반 삼제요법에 실패한 환자를 대상으로 7일간 VPZ 기반 MNZ 삼제요법은 PPI를 기반으로 하였을 때 보다 우월하였다(ITT 90% vs. 85%, P=0.045; PP 96% vs. 91%, P=0.008) [54]. PPI 기반 표준삼제요법과 VPZ 기반 표준삼제요법에 실패한 군을 동일하게 PPI 기반 MNZ 삼제요법으로 구제한 결과 양 군 간에 차이가 없어 VPZ을 사용하고 실패하더라도 후속적인 구제 요법에는 불이익이 없는 것으로 나타났다[55].
9. 프로바이오틱스
10. 백신과 새로운 시도
헬리코박터 파일로리 백신 개발을 위한 한 개의 최근 연구에서는 VacA, CagA, neutrophil-activating protein의 3가지 종류의 항원으로 구성된 백신을 시도하였는데, 백신에 의하여 강력한 체액성 면역 반응만 유발하였고 헬리코박터 파일로리 제균율을 상승시키지 못하였다[57]. 이집트의 한 연구에서 혈중 25 hydroxyvitamin D 농도가 제균 실패군에서 유의하게 낮아 vitamin D 결핍자(<20 ng/mL)에 대하여 vitamin D를 보충해주고 제균 치료를 시작하는 것이 제안되었다[62]. 발효유의 유청 단백질로부터 얻은 소 락토페린은 보조적으로 항균 특성을 가지는데, 투여 농도에 따라 성장 억제에서 사멸까지도 유도하였고[63], LFX 기반 삼제요법에 보조적으로 사용하였을 때 락토페린 추가군에서 제균율이 높았다(96% vs. 75%) [63]. 기타 key lime이 효과가 있었다는 보고가 있고[50], 국내에서는 병용 금기로 되어있는 simvastatin과 CLR의 조합이 제균율을 높였다는 연구도 있다[64].
11. 순응도
약제 복용의 순응도는 제균 성공의 성패를 좌우할 수 있다. 순응도 향상을 위하여 최근 연구된 투약 방법으로는 하루 1회 투여법과 단일제형 캡슐법이 있다. 하루 1회 투여법은 태국과 이란에서 보고되었는데, 태국에서 LFX 750 mg, CLR 1 g, rabeprazole 60 mg, BMT 1,048 mg을 하루 1회, 7일 또는 14일간 투여하였고 각각의 제균율은 84%, 94%로 유의한 차이는 없었다[67]. 이란에서 esomeprazole 40 mg, tinidazole 1 g 그리고 LFX 500 mg 하루 1회 복용과 STT의 14일 투약을 비교한 연구에서 제균율은 유의한 차이가 없었고 순응도가 유의하게 개선되었다[68]. 이 연구에서 제균 실패의 독립 위험인자는 치주염과 복약 순응도였다[68].
결 론
전 세계적으로 헬리코박터 파일로리 제균에 대한 항생제 내성이 문제가 되고 있다. 이를 극복하기 위하여 최근까지 항생제 감수성 검사를 통한 치료 약제의 선택, 해당 지역에 적합한 경험적 치료 조합 선정, 고용량 AMX을 이용한 이제요법, 항생제 내성이 적은 RFB, SFX 사용 등에 대한 데이터가 계속 보고되고 있고, 최근 PPI보다 산분비 억제력이 뛰어나다고 보고된 칼륨 경쟁적 산분비 억제제의 헬리코박터 파일로리 제균에 대한 역할이 관심을 모으고 있다. 순응도를 높이기 위하여 처방을 단순화하고 복약이 간편한 제형을 개발하고 있으며, 기타 항생제를 직접 점막에 도포하는 등의 새로운 치료법이 개발되어 연구 중이다.